
What the June Jobs Report Means for Fed Monetary Policy
53 mins ago

The oral targeted therapies that dominate B-cell malignancy treatment carry a structural limitation embedded in their own pharmacology: a proportion of patients will, over time, either develop resistance or become unable to tolerate them, and that failure point is not an edge case but a predictable feature of the drug class. BTK inhibitors, now a US$12.0 billion global market, work until resistance mutations or intolerance force patients off them. That ceiling is continuously replenishing a funnel of patients whose disease has outgrown the most widely prescribed drug class in blood cancer.
For those patients, the clock accelerates. They arrive at the next treatment decision heavily pre-treated, often with biologically aggressive disease, and the conventional autologous CAR-T option, where a patient’s own T cells are collected and engineered, demands a manufacturing window measured in weeks that many patients’ disease trajectories cannot accommodate.
What follows is an analytical breakdown of why the allogeneic off-the-shelf design may be structurally advantaged for this specific population, what the azer-cel Phase 1b data have shown so far about efficacy and tolerability across multiple B-cell malignancy subtypes, and what the opening of Cohort 3, the first combination arm pairing allogeneic CAR-T with a BTK inhibitor in BTKi-relapsed patients, means in practice for investors tracking Imugene (ASX: IMU).
BTK inhibitors block Bruton’s tyrosine kinase (BTK), a protein within the B-cell receptor signalling pathway that malignant B cells depend on for survival. Remove that signal, and the cancer cells lose a critical growth driver. The drug class, which includes ibrutinib, acalabrutinib, zanubrutinib, and pirtobrutinib, has become the established standard of care across four distinct B-cell malignancy types:
The global BTKi market is valued at around US$12.0 billion based on 2025 figures cited in an Imugene ASX announcement dated 22 May 2026. Different sources may report different estimates; the figure is presented to convey the scale of the treated patient population, not as a commercial projection for azer-cel.
That scale matters because the drug class carries a predictable biological ceiling operating through two distinct mechanisms. The first is acquired molecular resistance: mutations emerge within the BTK gene, most commonly at the C481S position and nearby sites, or within downstream signalling molecules such as PLCγ2, restoring the cancer cell’s ability to propagate despite the drug’s presence. The second mechanism is treatment discontinuation driven by intolerance, where cumulative toxicity or side-effects compel patients to stop therapy independently of whether the drug is still suppressing disease.
Peer-reviewed findings on BTK resistance mechanisms in CLL confirm that C481S mutations and downstream PLCγ2 escape variants are the dominant molecular drivers of acquired resistance, a pattern that holds across covalent and noncovalent inhibitor generations alike.
Both mechanisms feed the same funnel: a structurally large, continuously replenishing cohort of BTKi-relapsed or refractory patients who urgently need a next-line therapy. That cohort is the foundation of the entire clinical and investment thesis that follows.
Conventional autologous CAR-T therapy uses the patient’s own T cells. The manufacturing process follows a fixed sequence:
The total vein-to-vein time under current commercial processes spans approximately 2-4 weeks. That interval is not medically inert. Tumour biology advances regardless of where the patient is in the manufacturing queue, and for individuals who are already heavily pre-treated and have exhausted multiple prior lines, the weeks between cell collection and infusion carry real clinical weight. Documented rates of manufacturing failure and disease progression during the wait period account for a meaningful portion of patients who never reach infusion at all.
According to a Diamond Equity Research note dated 18 June 2026, azer-cel’s anticipated operational delivery window runs to approximately 3-5 days from treatment decision to infusion, though actual turnaround times may vary. The comparison that matters for this patient population is not an abstract scheduling preference: when disease is advancing in a patient who has already exhausted BTKi therapy, the distinction between a days-long and a weeks-long wait determines whether treatment arrives when it can still do its job.
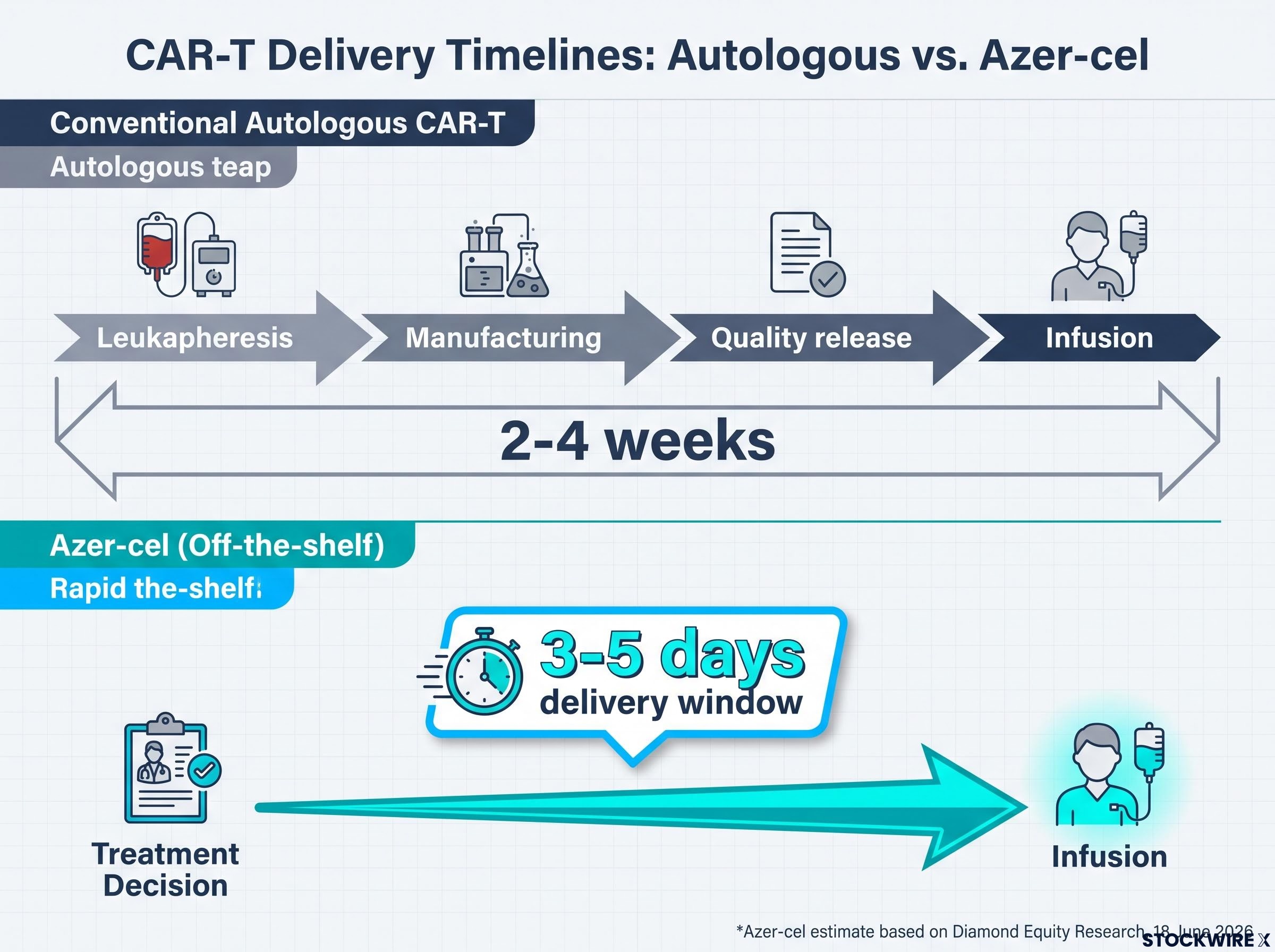
Because azer-cel is manufactured from healthy donor T cells and stored ready for use, there is no patient-specific manufacturing step. The product is pre-made, shipped on demand, and administered at the treatment site. That is the structural logic of the off-the-shelf model, and it is most consequential precisely for the post-BTKi population where time and T-cell fitness are most constrained.
The combination of azer-cel with a BTK inhibitor is not a case of replacing one therapy with another. It is a distinct clinical hypothesis: that BTK inhibition, even in patients whose disease has progressed beyond what BTKi can control alone, may serve a different biological function when layered alongside CAR-T.
The immunomodulatory hypothesis works like this. Emerging preclinical and early clinical findings suggest that BTK inhibition may reduce immunosuppressive signalling within the tumour microenvironment, the cellular and molecular ecosystem surrounding the cancer, in ways that could create more favourable conditions for engrafted CAR-T cells to expand and persist. The evidence points to effects on regulatory cell populations and myeloid and T-cell subsets that may collectively lower the barriers engineered T cells face after infusion.
Tumour microenvironment remodelling by BTK inhibitors is the mechanism under investigation in Cohort 3: preclinical findings suggest that ibrutinib-class agents may reduce the immunosuppressive cell populations that otherwise limit how effectively engrafted CAR-T cells can expand, persist, and sustain cytotoxic activity after infusion.
The role allocation in Cohort 3 reflects this:
The distinction matters for investors. The thesis here is not that azer-cel substitutes for BTKi therapy, but rather that it may operate as a complementary agent alongside BTKi in patients whose disease has already advanced past what BTKi can manage on its own. Framed that way, the commercial and clinical position shifts from salvage alternative to potentiating partner, a meaningfully different basis for thinking about the asset’s total addressable opportunity.
The combination rationale is based on emerging evidence and company communications. Cohort 3 is investigational and designed to test whether this biological hypothesis translates clinically.
Results from the Phase 1b programme cover 24 CAR-T-naive evaluable patients enrolled across six B-cell malignancy subtypes, with the most current data presented at ASCO 2026.
The basket trial design simultaneously evaluates azer-cel across multiple B-cell malignancy subtypes within a single protocol, an adaptive structure that allows the programme to generate registrational-quality signals across indications where BTKi forms the standard of care while preserving the flexibility to pivot resources toward the cohorts producing the strongest responses.
Among the 14 evaluable patients with indolent subtypes, treatment produced a combined overall response rate (ORR), meaning the proportion of patients whose disease measurably shrank or cleared, of 93%.
The per-indication breakdown shows consistency across the subtypes where BTKi is standard of care:
| Indication | Evaluable patients | ORR | Complete responses |
|---|---|---|---|
| CLL/SLL | Assessed in March 2026 data cut | 100% | Per data cut |
| MZL | 6 | 83% | 4 complete responses |
| Combined indolent subtypes | 14 | 93% | Across subtypes |
The MZL data reflect the updated figures from the Diamond Equity Research note dated 18 June 2026, revised upward from 80% ORR in the earlier data cut.
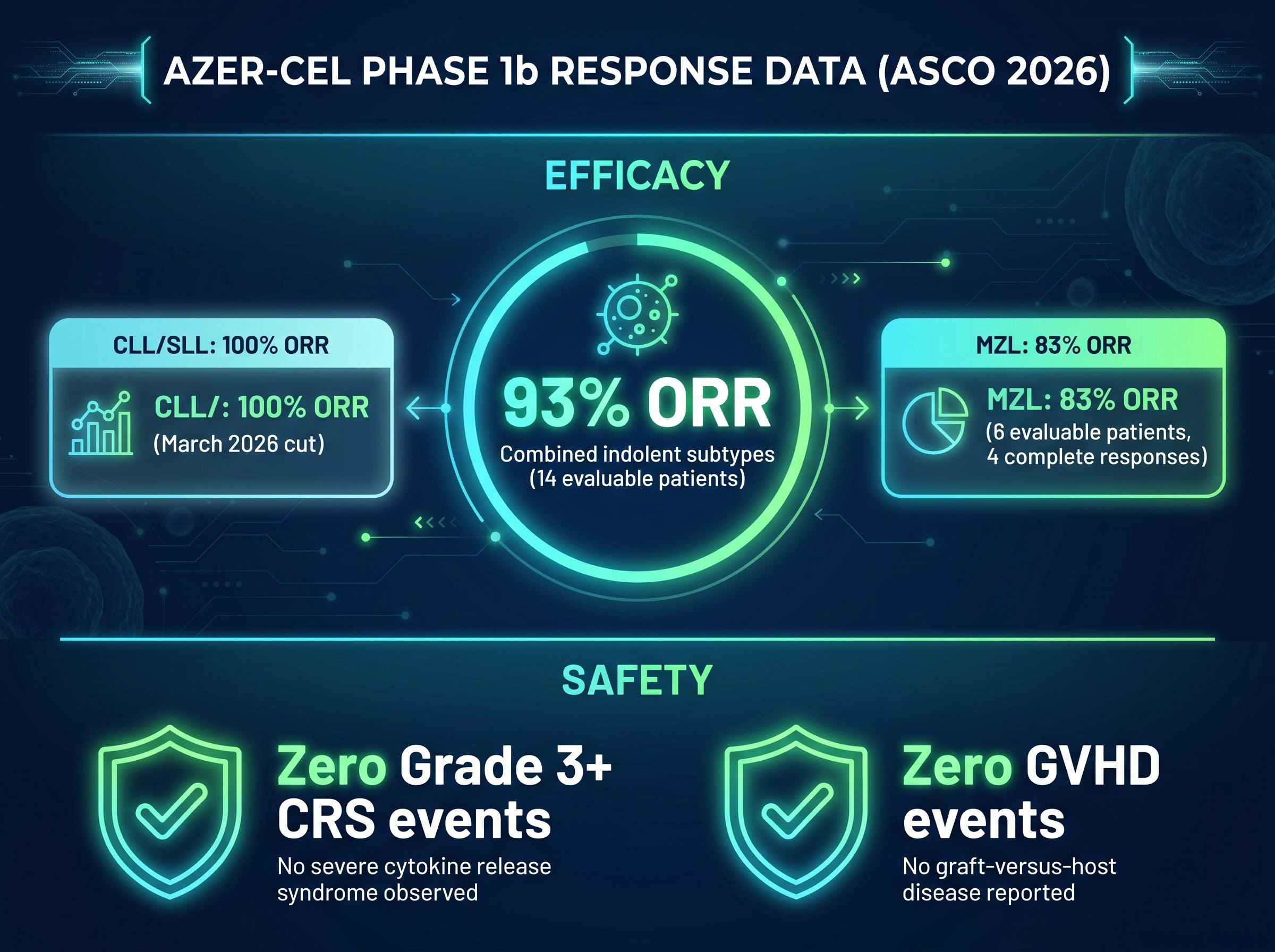
The safety profile across the complete Phase 1b programme is equally notable:
The FDA granted Fast Track designations for relapsed/refractory CLL/SLL and relapsed/refractory MZL, per an Imugene ASX announcement dated 9 June 2026, providing regulatory scaffolding and rolling review eligibility ahead of any registrational submission.
The 93% combined ORR across indolent subtypes confirms that the platform is active in precisely the indications where BTKi forms the standard of care, which means Cohort 3 represents a progression of an already-working platform into harder ground, not an unanchored speculative leap. That said, these results remain preliminary and do not yet supply the durability data, head-to-head comparisons, or patient-volume evidence that regulators require before approving a new therapy.
On 28 May 2026, the first Cohort 3 patient received their infusion at Baylor University Medical Center in Texas, as disclosed by Imugene in an ASX announcement. That patient carried an MCL diagnosis with documented prior BTKi exposure, making them representative of the combination arm’s target population.
The trial network supporting Cohort 3 is distributed across 15 investigational sites in two countries:
Registry data for Cohort 3 may not yet be fully captured in ClinicalTrials.gov; the enrolment milestone is reported on the basis of company announcements and third-party analyst coverage. The approximately 3-5 day delivery window is particularly relevant for this heavily pre-treated population given the clinical urgency characteristic of BTKi-relapsed disease.
The operational milestone is distinct from a clinical outcome. What followed, however, provided the first early clinical signals from the combination arm.
The first FL patient to enter the combination cohort, having previously progressed on BTKi therapy, was assessed at Day 28 and confirmed to have achieved a complete response, as reported by Imugene on 30 June 2026. The first MCL patient treated in the entire Phase 1b programme, who had also previously failed BTKi therapy, was likewise assessed at Day 28 and confirmed as a complete response, reported on 1 July 2026.
Two complete responses in the first two evaluable BTKi-relapsed patients are an early signal worth noting. But this cohort has only just opened. These data points are not sufficient on their own to draw conclusions about the combination’s efficacy. They are the first readings from an investigational arm that will need substantially more patients and longer follow-up before the hypothesis can be considered validated.
Complete responses in BTKi-relapsed patients at Day 28 assessments across two separate malignancy subtypes, FL and MCL, provide the earliest clinical indication that the combination arm is producing the depth of tumour clearance the monotherapy cohorts established as a benchmark, even in a population whose disease had already progressed beyond what BTKi alone could control.
Graft-versus-host disease has historically been the central immunological concern constraining allogeneic CAR-T adoption. When donor T cells are infused into a recipient, their native T-cell receptors (TCRs) can recognise the recipient’s tissues as foreign and mount an immune attack. This is the biological basis of GVHD, and it is the reason allogeneic cell therapy has carried a credibility burden that autologous approaches do not.
Azer-cel’s platform is engineered to address this at the manufacturing stage, not retrospectively through immunosuppression. The ARCUS genome-editing technology, developed by Precision BioSciences, employs a non-integrating adeno-associated virus (AAV) vector to insert the CD19-targeting CAR construct at a specific genomic address: the TRAC locus, which encodes the T-cell receptor alpha constant region.
The insertion point is the mechanism. Placing the CAR construct at the TRAC locus simultaneously disables the donor cell’s endogenous TCR, because the act of integration at that site breaks the receptor’s structural continuity. Once the native TCR is rendered non-functional, the donor cells no longer carry the machinery needed to mount an attack against the recipient’s own tissues.
Through the ASCO 2026 presentations and associated Imugene ASX announcements, not a single GVHD event has been recorded anywhere in the Phase 1b programme. This clean record is consistent across every cohort reported to date.
Zero Grade 3 or higher CRS events complement the GVHD safety finding, reinforcing a tolerability profile that, if it holds in the combination arm, supports the allogeneic model’s viability in a broad patient population.
The zero-GVHD record is not a marketing claim. It is clinical evidence that the TRAC locus engineering approach is functioning as designed, which is the structural prerequisite for the off-the-shelf model to hold up under scrutiny. For investors, this reframes the GVHD question: it is no longer an open theoretical concern but a hypothesis that has been tested across a growing patient cohort and confirmed at every point so far.
The Cohort 3 thesis for Imugene (ASX: IMU) will be tested through four specific, trackable milestones, listed in order of clinical immediacy:
| Watchpoint | What it tests | Why it matters |
|---|---|---|
| Combination arm tolerability | Whether zero Grade 3+ CRS and zero GVHD hold with BTKi added | Safety profile is the prerequisite for the combination thesis |
| Initial response data | ORR and response depth in BTKi-relapsed patients | Determines if the platform retains activity in the hardest-to-treat cohort |
| Enrolment pace | Recruitment speed across 15 sites | Controls the timeline for data readouts |
| Regulatory designations | Additional FDA Fast Track or Breakthrough Therapy designations | Signals agency engagement with the combination approach |
Each watchpoint either reinforces or complicates the thesis that azer-cel can work in the post-BTKi population. What you assign weight to depends on which dimension of the thesis you are most uncertain about: safety, efficacy, execution, or regulatory pathway.
Investing in development-stage biotechnology companies involves a real risk of losing the entire capital invested. Nothing in this analysis constitutes financial or investment advice. These watchpoints represent future events, not validated outcomes.
The azer-cel programme has followed a coherent clinical logic across three stages:
Cohort 3 is the question the monotherapy cohorts earned the programme the right to ask. It is not a separate speculative leap but the next step in a progression where each stage’s data informed the next stage’s design.
The US$12.0 billion BTKi market provides population-scale context for the Cohort 3 patient universe. FDA Fast Track designations for CLL/SLL and MZL are already in place, providing regulatory scaffolding ahead of Cohort 3 data. The early complete responses in the first two evaluable BTKi-relapsed patients are encouraging but preliminary.
The point at which a single patient has been dosed and the point at which enough data exist to move a development thesis forward are separated by considerable time, patient numbers, and follow-up, and that interval is where the genuine uncertainty resides.
That is where the analysis must be honest. The development arc’s internal coherence is the strongest argument for taking Cohort 3 seriously as a thesis. Yet the journey from initial signals to a registrational dataset is long, and the clinical and regulatory risk embedded in that journey is substantial. Investors who track the evidentiary logic connecting each programme stage can place each future data readout in its proper context, which is the difference between following a thesis with comprehension and simply reacting to headlines.
This article is for informational purposes only and should not be considered financial advice. Investors should conduct their own research and consult with financial professionals before making investment decisions. All forward-looking elements, including Cohort 3 data, BTKi-combination results, and regulatory trajectories, remain investigational and carry substantial clinical and regulatory risk.
Allogeneic CAR-T therapy uses engineered T cells from a healthy donor that are manufactured in advance and stored ready for use, whereas autologous CAR-T requires extracting, engineering, and expanding the patient's own T cells, a process that takes approximately 2-4 weeks. The off-the-shelf model eliminates that manufacturing window, which is clinically significant for heavily pre-treated patients whose disease cannot wait.
BTK inhibitor resistance occurs when mutations, most commonly at the C481S position in the BTK gene or in downstream signalling molecules like PLCγ2, allow malignant B cells to continue proliferating despite the drug's presence. Because resistance is a predictable feature of the drug class rather than an edge case, it continuously produces a large cohort of patients who need an effective next-line therapy, which is exactly the population azer-cel's Cohort 3 is designed to treat.
Across 14 evaluable patients with indolent B-cell malignancy subtypes, azer-cel produced a combined overall response rate of 93% as of the ASCO 2026 data presentation. Per-indication results include a 100% ORR in CLL/SLL and an 83% ORR across 6 evaluable MZL patients, with 4 complete responses.
Cohort 3 is the first arm pairing azer-cel with a BTK inhibitor in patients whose disease has already progressed on BTKi therapy, testing whether the combination produces better outcomes than either agent alone. The first two evaluable patients both achieved complete responses at Day 28, but the cohort has only just opened and needs substantially more patients and follow-up before the efficacy hypothesis can be considered validated.
The ARCUS genome-editing system inserts the CD19-targeting CAR construct at the TRAC locus in donor T cells, and the act of integration at that site breaks the structural continuity of the donor cell's native T-cell receptor, rendering it non-functional. Without an active TCR, the donor cells cannot recognise the recipient's tissues as foreign, which is why the Phase 1b programme has recorded zero GVHD events across all cohorts through ASCO 2026.




