
Morningstar vs Markets: a 125-Point Gap in the US Rate Outlook
40 mins ago
For most patients diagnosed with diffuse large B-cell lymphoma (DLBCL), the most common form of aggressive non-Hodgkin lymphoma, front-line therapy works. The disease is frequently curable at the first attempt. That fact makes what happens next, for the patients it does not cure, structurally different from a simple progression through treatment lines.
When DLBCL relapses after two or more prior therapies, the clinical arithmetic shifts. The standard tools, transplant, autologous CAR-T cell therapy (where a patient’s own immune cells are engineered to attack cancer), and salvage chemotherapy, are either already spent or structurally unavailable. What remains offers modest response rates and short-lived benefit.
A systematic review of third-line DLBCL outcomes published in May 2024 quantified the modest response rates and short survival durations that characterise this population, providing the empirical baseline against which any new programme’s early signals must ultimately be judged.
This analysis frames the treatment gap in third-line or later (≥3L) DLBCL as a structural problem, then unpacks what the early azer-cel data from ASCO 2026 actually demonstrate, what the November 2025 FDA regulatory alignment means in practical terms, and which questions remain open. Here is the framework for weighing early-stage oncology data against the size of the clinical need it targets, so that neither optimism nor scepticism runs ahead of the evidence.
The distinction matters. A patient relapsing after first-line therapy still has escalation options available: a second regimen, potentially a stem cell transplant, potentially CAR-T. A patient arriving at the ≥3L threshold is not simply further along the same path. They are operating outside the system of options that produced the field’s best outcomes.
The population reaching third line is disproportionately older, carrying more comorbidities, or harbouring disease that proved refractory to prior chemotherapy. These are not incidental characteristics. They are the reasons the standard escalation pathways, designed for fitter, treatment-responsive patients, become unavailable by definition.
Three independent barriers converge at this threshold, and understanding them separately is what makes the treatment gap legible:
The convergence of all three barriers at the ≥3L threshold means this is a population for whom the system’s strongest tools have already been deployed or are structurally unavailable. They are not awaiting the next step in a treatment ladder. The ladder has ended.
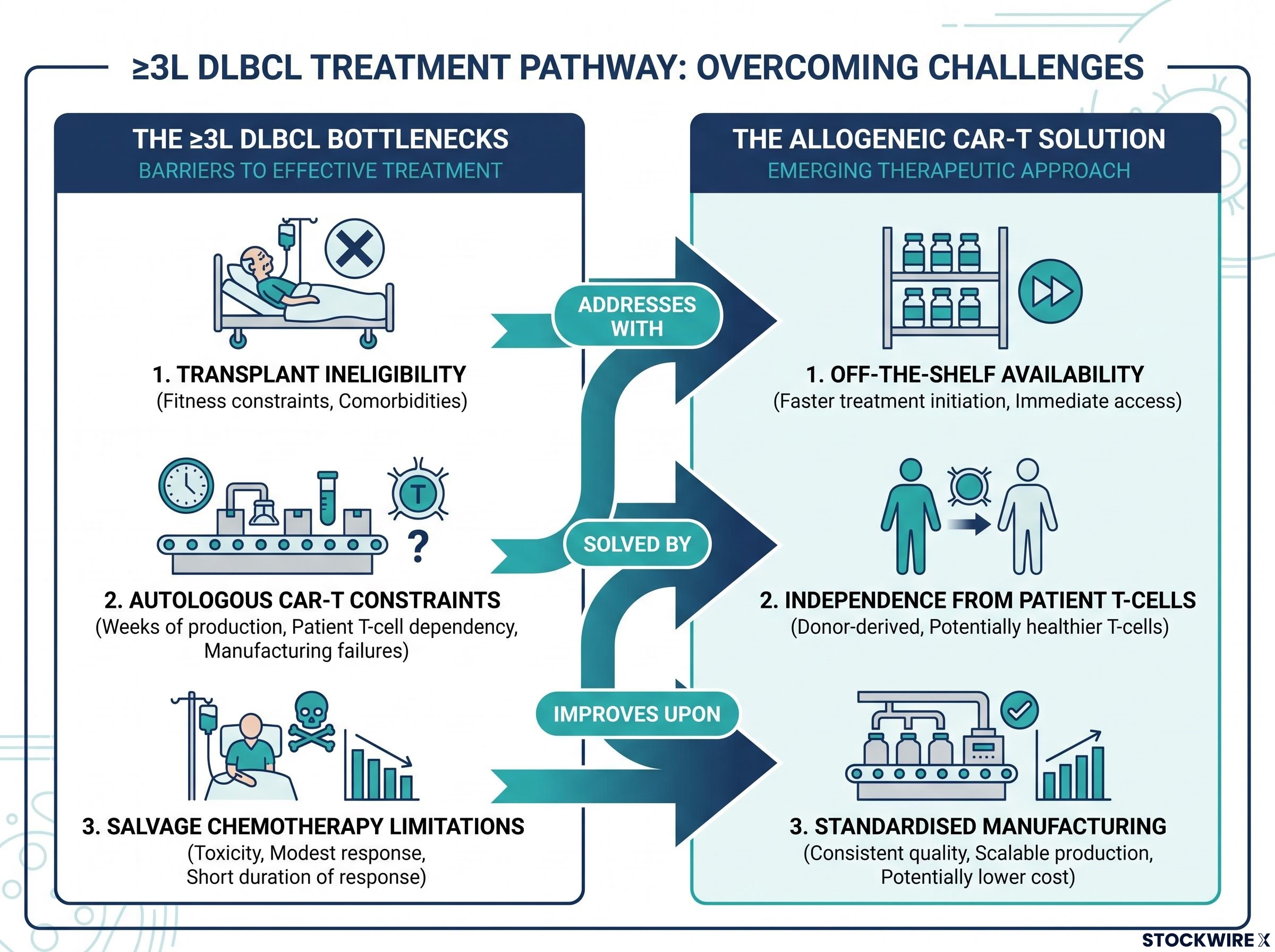
The theoretical case for allogeneic (donor-derived, “off-the-shelf”) CAR-T therapy maps directly onto the constraints that define the ≥3L DLBCL population. Where autologous CAR-T depends on the patient’s own T-cells, allogeneic products are manufactured from healthy donor cells in advance, which addresses three specific bottlenecks:
The logic is sound. The track record is not yet there to match it.
The unresolved tension: Multiple allogeneic CAR-T programmes have struggled to translate encouraging Phase 1 signals into late-stage data demonstrating the depth and durability of response that approved autologous products have achieved in eligible patients. Whether logistical advantages can produce equivalent clinical outcomes remains the central open question for the field.
Peer-reviewed analysis of allogeneic CAR-T clinical translation challenges in B-cell malignancies identifies the gap between Phase 1 response signals and late-stage durability as the field’s central unresolved problem, the same pattern that frames the analytical context for evaluating any single allogeneic programme’s early data.
That pattern, early promise followed by translation difficulty, is the analytical context for evaluating any single allogeneic programme’s data, including azer-cel’s.
Azer-cel (azercabtagene zapreleucel) is an allogeneic CD19-directed CAR-T therapy developed by Imugene, currently in Phase 1b evaluation across relapsed/refractory B-cell malignancies including DLBCL. The ASCO 2026 dataset was drawn from a Phase 1b basket trial enrolling 25 patients who had not previously received CAR-T therapy. Participants were heavily pre-treated: 60% carried primary refractory disease (meaning their DLBCL never responded to initial treatment), participants had received a median of 2 prior lines of therapy, and 56% had prior BTK inhibitor exposure.
Two DLBCL-specific data snapshots appear in the available evidence, and both deserve direct presentation rather than selective citation.
| Data Snapshot | DLBCL Patients Enrolled | Evaluable | ORR | Responses |
|---|---|---|---|---|
| ASCO 2026 updated dataset | Not specified separately | 6 | 67% | 1 CR, 3 PR |
| Separately reported data cut | 10 | 9 | ~44% | 3 CR, 1 PR |
The overall response rate (ORR, the proportion of patients whose tumours shrank meaningfully) ranges from 44% to 67% depending on which cohort snapshot you read. A complete response (CR) means no detectable disease remains; a partial response (PR) means significant tumour reduction short of complete disappearance. The two figures reflect different data cuts or timepoints rather than contradictory results. In cohorts this small, the addition or subtraction of even one or two patients changes the percentage substantially. This kind of snapshot variability is expected in early-phase oncology, not a signal of data quality problems.
Unverified figure: Expanded cohort data incorporating low-dose interleukin-2 have been reported to show a 75% ORR and 55% CR rate. This figure has not been independently confirmed and should be treated accordingly.
All efficacy figures must be interpreted in the context of early-stage, small, uncontrolled cohorts. These findings are preliminary and not indicative of regulatory approval or predictive of outcomes at scale.
The safety picture for azer-cel requires reading at the right level of granularity, because the aggregate numbers and the DLBCL-specific numbers tell different stories.
Looking at the full 25-patient mixed-malignancy cohort, the headline is reassuring on one front: cytokine release syndrome (CRS) events of Grade 3 severity or above were absent from the dataset. CRS, an inflammatory response triggered when engineered cells activate in the body, occurred at Grade 1-2 severity in approximately 42% of treated patients. All events were manageable.
The more clinically important signal sits in the ICANS data, and it requires separating two different denominators:
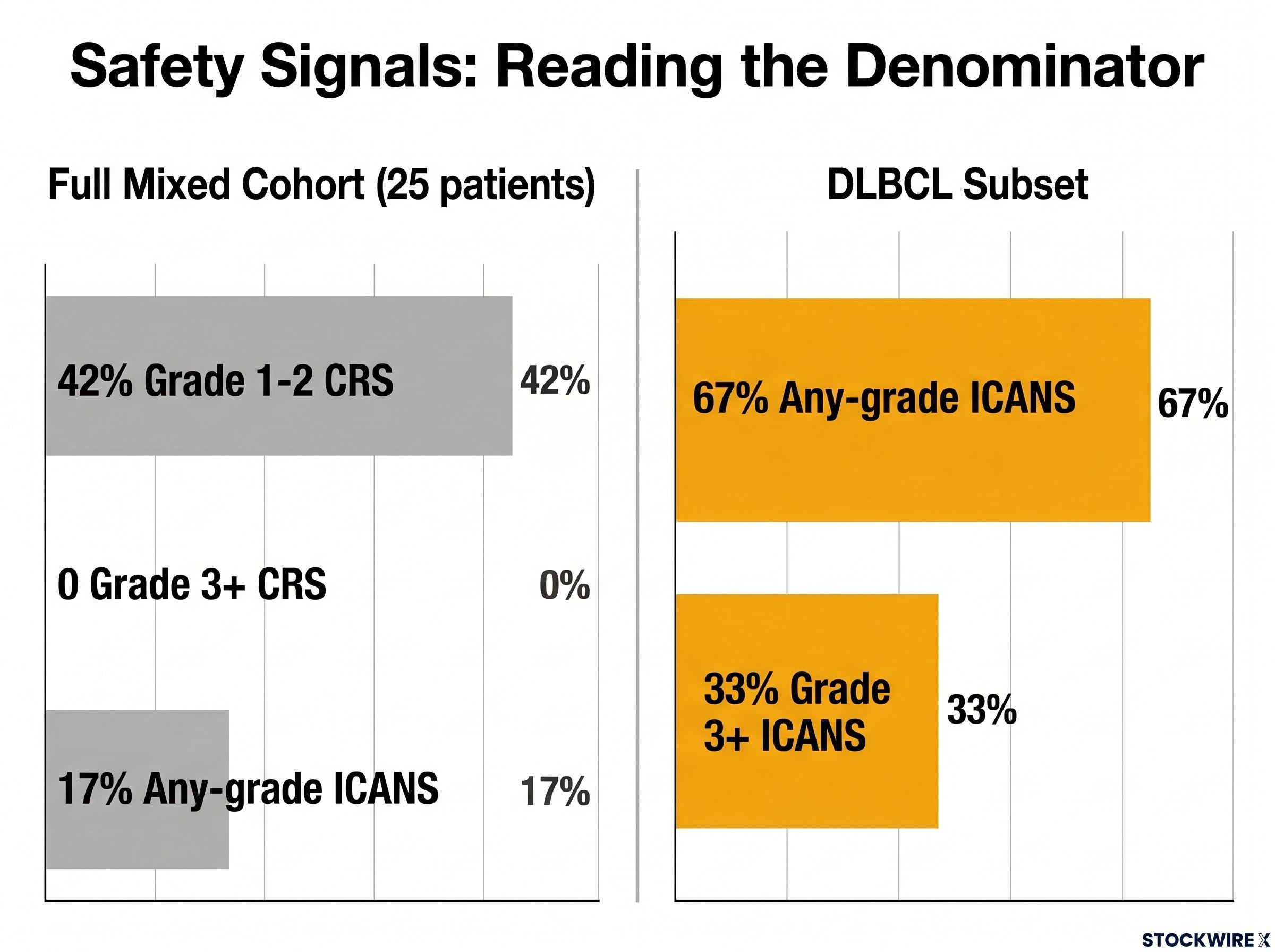
The DLBCL-specific ICANS rate is notably higher than the aggregate figure. These are not contradictory data points; they reflect different denominators. The DLBCL subset versus the full mixed-malignancy population. But the concentration of ICANS in DLBCL patients specifically is a finding that raises a clinical question rather than providing reassurance. The term “manageable” in the context of intensive monitoring within a small Phase 1b cohort does not automatically translate to a manageable profile at the scale of a registrational trial. DLBCL-specific monitoring will matter as the programme advances.
This article is for informational purposes only and should not be considered financial advice. Investors should conduct their own research and consult with financial professionals before making investment decisions.
Two regulatory milestones frame azer-cel’s development pathway. Both are meaningful. Neither is what they are sometimes presented as.
Imugene received FDA Fast Track designation for azer-cel in relapsed/refractory DLBCL. A Fast Track designation formally recognises that a therapy addresses a serious condition with an unmet medical need. It facilitates more frequent communication with the FDA and may support expedited review. It does not imply the therapy works or that approval is likely.
In November 2025, following a Type C meeting (a formal written-response meeting between a drug developer and the FDA), the FDA confirmed that it and Imugene had reached agreement on the key design elements of a registration-enabling study for azer-cel in ≥3L DLBCL. A Type C meeting addresses specific development questions. The outcome here was agreement on trial design and endpoints (the specific health outcomes the trial will measure to determine whether the treatment works) for a study in patients who have received at least two prior lines of therapy.
FDA institutional capacity has deteriorated materially since 2025, with more than 1,300 staff departures creating unpredictable approval backlogs particularly in cell and gene therapies; that context sits behind any assessment of how reliably a Type C meeting agreement translates into an on-schedule registrational programme.
The distinction that matters: Fast Track designation and Type C meeting alignment are process milestones. They confirm that the regulatory route is open and the development plan is coherent. They do not tell you the destination is assured. For anyone evaluating a clinical-stage programme, the gap between “the pathway exists” and “approval is likely” is one of the most practically important distinctions to maintain.
These statements are speculative and subject to change based on market developments and company performance. Past performance does not guarantee future results.
What ASCO 2026 has provided for azer-cel are early-phase findings drawn from small, uncontrolled patient cohorts. This is not a criticism of the programme. Phase 1b studies are designed to establish safety, identify dosing, and generate preliminary efficacy signals. They are not designed to answer the questions that matter most for determining whether a therapy will ultimately reach patients at scale.
Three open questions define what the data structurally cannot tell you at this stage:
A 67% ORR in 6 evaluable patients is a data point worth watching. It is not a conclusion worth acting on. The questions that Phase 2/3 trials are designed to answer, durability, comparative efficacy, safety at scale, are the ones that will actually determine this programme’s clinical significance.
The treatment gap in ≥3L DLBCL is structural, not circumstantial. It exists because three independent barriers, transplant ineligibility, autologous CAR-T constraints, and salvage chemotherapy’s diminishing returns, converge at the same point in the treatment pathway. That gap is real regardless of what any individual programme’s data show.
Azer-cel currently occupies a specific and clearly defined position within that gap. The unmet need is recognised by the FDA. The regulatory pathway is open following November 2025 alignment. The early efficacy signals from ASCO 2026, whether read as 67% or 44% ORR depending on the cohort snapshot, are preliminary findings from small uncontrolled studies. The safety profile raises a DLBCL-specific ICANS question that will require larger cohorts to resolve.
The three variables that will determine whether this programme, or any allogeneic CAR-T approach, can close the ≥3L DLBCL gap are now clearly defined: registrational trial results on response durability, comparative trial design demonstrating where allogeneic therapy sits relative to available options, and DLBCL-specific safety data at a scale that moves beyond early-phase monitoring. Until those data arrive, the analytical position is calibrated, not conclusive. The evidence warrants attention, not conviction, in either direction.
For investors wanting to connect the clinical evidence to a capital markets framework, our deep-dive into Imugene’s valuation against allogeneic CAR-T peers examines the milestone payment obligations to Precision BioSciences and the dilution risk that each independently shapes whether the current valuation gap narrows.
Third-line DLBCL refers to diffuse large B-cell lymphoma that has relapsed or progressed after at least two prior therapies. At this stage, the three main salvage options (stem cell transplant, autologous CAR-T, and chemotherapy) are either already spent or structurally unavailable due to patient fitness, disease refractory status, or manufacturing constraints, leaving most patients with very limited options.
In a Phase 1b cohort of 6 evaluable DLBCL patients, azer-cel produced a 67% overall response rate including 1 complete response and 3 partial responses; a separately reported data cut of 9 evaluable patients from a 10-patient cohort showed approximately 44% ORR with 3 complete responses, reflecting different data timepoints rather than contradictory results.
Fast Track designation confirms that the FDA recognises azer-cel addresses a serious condition with an unmet medical need, enabling more frequent FDA communication and potentially expedited review, but it does not imply the therapy works or that approval is likely.
ICANS (immune effector cell-associated neurotoxicity syndrome) is a neurological side effect of CAR-T therapies that can include confusion, speech difficulty, or seizures. In the azer-cel DLBCL subset, 67% of patients experienced any-grade ICANS and 33% experienced Grade 3 or higher events, a notably higher rate than the 17% seen across the broader mixed-malignancy cohort, raising a disease-specific safety question that larger trials will need to resolve.
The November 2025 Type C meeting resulted in FDA agreement on the key design elements and endpoints for a registration-enabling study of azer-cel in patients with three or more prior lines of DLBCL therapy, confirming the regulatory pathway is open, though it does not guarantee approval or an on-schedule programme given current FDA institutional pressures.




