
Citi Puts Memory Supply Above Chip Design in AI Stock Rankings
26 mins ago

A 93% response rate in a patient population that has never received CAR-T therapy before. That figure, drawn from oral presentation data at the 2026 ASCO Annual Meeting, is the number Imugene investors should be sitting with as the programme turns toward its next phase.
The result comes from a subgroup that has historically been underserved by CAR-T development: patients with indolent B-cell lymphomas, cancers defined not by rapid aggression but by a chronic, relapsing course spanning years or even decades. Following the ASCO presentation, the US Food and Drug Administration (FDA) granted Fast Track designation to azer-cel for two of these indolent subtypes: relapsed/refractory chronic lymphocytic leukaemia/small lymphocytic lymphoma (CLL/SLL) and relapsed/refractory marginal zone lymphoma (MZL). Three converging signals now point to indolent disease as the programme’s emerging registrational focus: the highest response rates in the ASCO dataset, FDA engagement directed at indolent subtypes specifically, and the commercial durability of a chronic patient population cycling through treatment over time.
Here is a clear framework for understanding what the indolent lymphoma setting actually means clinically, how azer-cel’s data compares across subtypes, what Fast Track designation does and does not signal, and which forward-looking variables will determine whether this becomes a genuine registrational opportunity.
Indolent B-cell lymphomas are slower-progressing blood cancers. Where aggressive subtypes like diffuse large B-cell lymphoma (DLBCL) move fast, demanding urgent clinical intervention, indolent disease operates on a different clock entirely. These cancers progress over years, sometimes decades, and the treatment journey reflects that tempo.
Four indolent subtypes are relevant to the azer-cel programme:
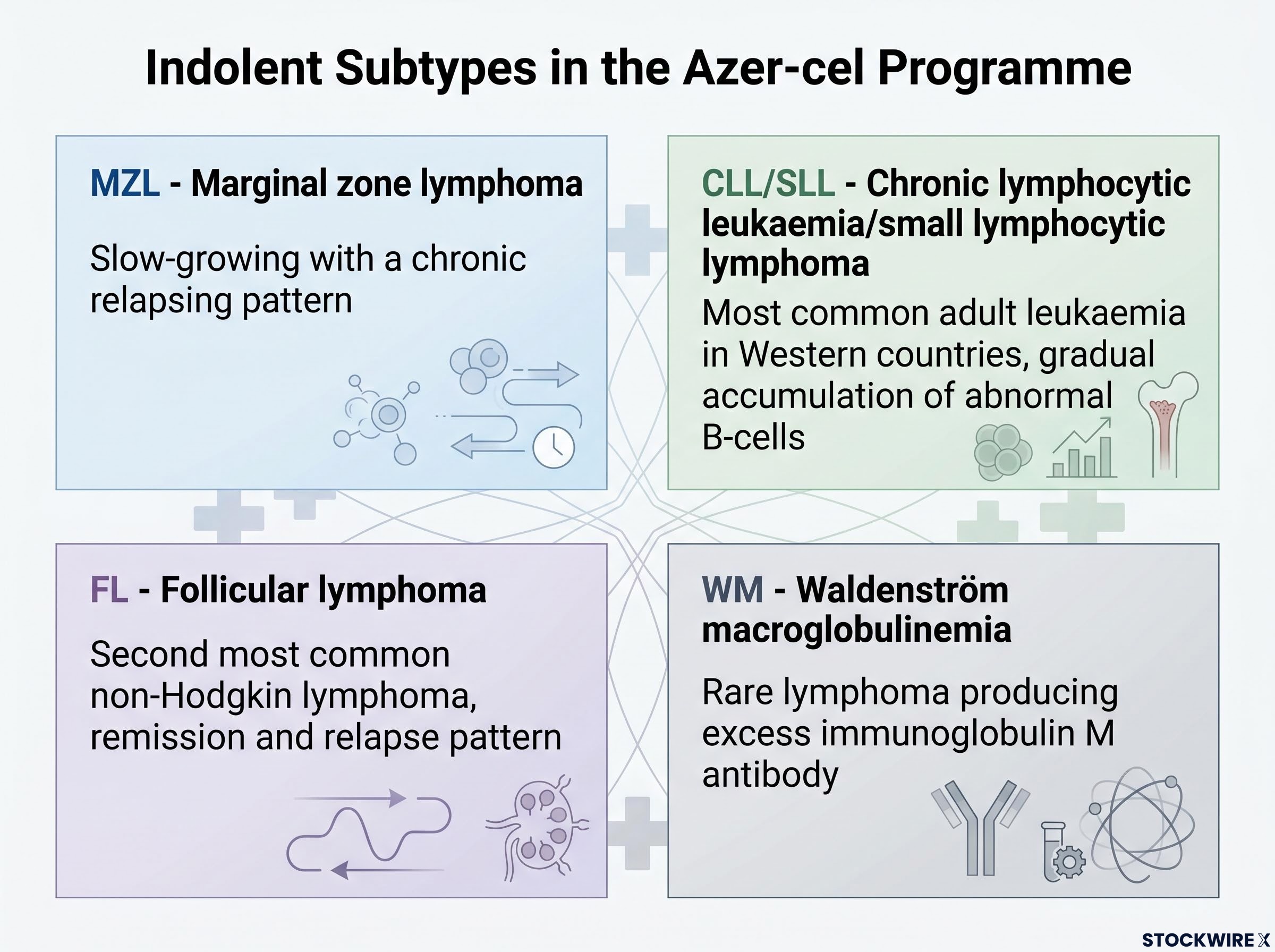
What connects these four subtypes is the relapse-and-retreat cycle. A patient receives a line of therapy, achieves remission or stabilisation, eventually relapses, and receives the next line. This cycle can repeat across a decade or more, with each relapse representing both a clinical challenge and a new point where treatment decisions are made. Prior treatment histories in this population frequently include BTK inhibitor therapy, bispecific antibodies, chemotherapy, and autologous stem cell transplant, all before any CAR-T exposure.
BTK inhibitor resistance creates a downstream patient population that is structurally aligned with azer-cel’s off-the-shelf delivery model: patients who have exhausted BTKi options need a next-line therapy available within days, not weeks, and the recently opened Cohort 3 at Baylor University Medical Center positions azer-cel directly at that clinical gap.
A CAR-T product entering the indolent space does not compete for a single treatment-line decision. It enters a patient population that will remain in active treatment cycling for years. That is a fundamentally different commercial proposition than aggressive disease, where the treatment window is defined by clinical urgency and a compressed timeline. The CAR-T-naive population in indolent lymphoma represents a large, addressable, first-entry opportunity in a chronic disease setting, and the durability of that opportunity is built into the biology of the disease itself.
The Phase 1b data presented at ASCO 2026 covered 24 efficacy-evaluable patients, all CAR-T naive, with a minimum of one to two prior lines of therapy. Several patients had received multiple prior lines including bispecific antibodies and autologous stem cell transplant. The abstract earned selection for oral presentation from a field of more than 8,500 submissions, an outcome determined by independent scientific peer review.
The ASCO 2026 dataset expanded on an earlier Phase 1b readout from March 2026, which showed 100% ORR across four evaluable CLL/SLL patients and an 80% response rate in MZL, establishing the foundational efficacy signal that the ASCO oral presentation built upon with a larger CAR-T-naive cohort.
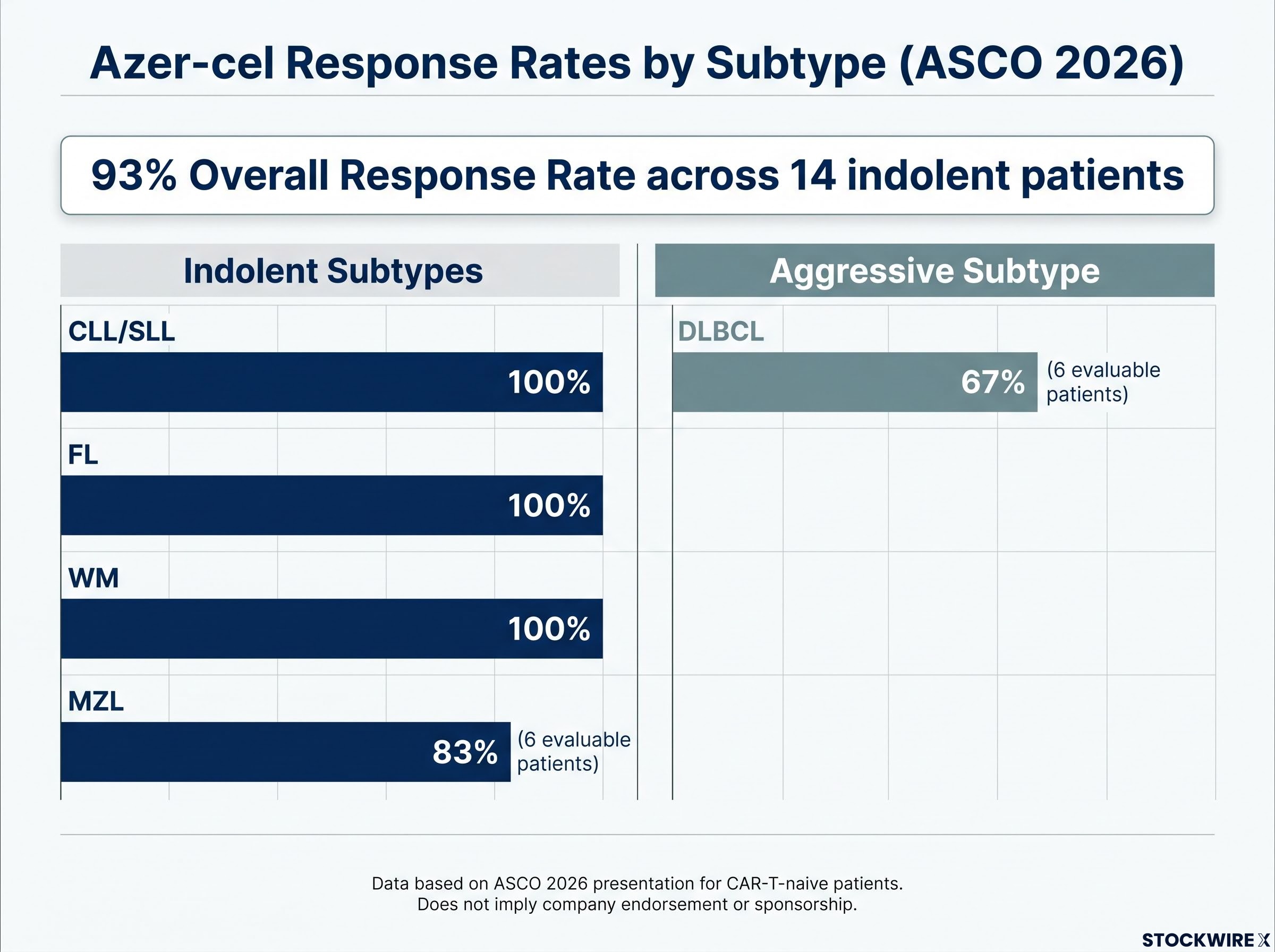
93% overall response rate across 14 evaluable CAR-T-naive indolent patients, ASCO 2026.
The subtype-by-subtype breakdown tells you where the signal is strongest:
| Subtype | Disease Category | Evaluable Patients | ORR | Response Detail |
|---|---|---|---|---|
| MZL | Indolent | 6 | 83% | 4 complete responses |
| CLL/SLL | Indolent | Included in 14 | 100% | CAR-T-naive cohort |
| FL | Indolent | Small n | 100% | Including 1 complete response |
| WM | Indolent | Small n | 100% | Including 1 partial response |
| DLBCL | Aggressive | 6 | 67% | 2 complete responses |
Two dataset caveats investors should hold alongside these figures:
The 93% combined overall response rate (ORR) across indolent subtypes, set against the 67% ORR in DLBCL within the same dataset, tells you that azer-cel’s strongest signal sits in the chronic, relapsing patient population. That is exactly where the FDA’s subsequent Fast Track designations landed.
In CAR-T therapy, efficacy without a manageable safety profile does not move a programme forward. Two adverse event categories matter most:
No CRS events of Grade 3 or higher were recorded. No GVHD cases have emerged in the dataset to date.
Across the 24 evaluable CAR-T-naive patients, according to Imugene ASX announcements dated 1 April and 22 May 2026, azer-cel recorded zero Grade 3 or higher CRS events and no cases of GVHD. In the allogeneic CAR-T context, where both risks are structurally present because the therapy uses donor cells rather than the patient’s own, these findings are not a minor footnote.
For investors, a clean safety signal at the Phase 1b stage is a prerequisite for efficient progression toward any registration-directed study. Regulators will require this profile to hold at larger scale before granting approval. Whether it does is one of the three forward-looking variables that will define the programme’s trajectory.
Following the ASCO presentation, the FDA granted Fast Track designation to azer-cel for relapsed/refractory CLL/SLL and relapsed/refractory MZL, according to a Diamond Equity Research note dated 18 June 2026. Fast Track is a regulatory programme designed for therapies that target serious conditions where current options fall short, and it opens four specific pathways for the developer:
The FDA Fast Track designation for CLL/SLL and MZL followed Phase 1b data showing 100% ORR in CLL/SLL patients and 83% ORR in MZL patients, with four complete responses, giving azer-cel regulatory scaffolding across both indolent indications before any expanded cohort data has been reported.
What Fast Track does not confer is equally important:
Three converging factors position indolent disease as the programme’s registrational centrepiece. First, the 93% combined indolent ORR versus 67% DLBCL ORR within the same dataset shows the strongest efficacy signal in the chronic, relapsing population. Second, the FDA’s Fast Track designations were directed at CLL/SLL and MZL rather than DLBCL, a distinction that reflects where regulatory attention is focused. Third, the extended, cyclical treatment course that characterises indolent lymphoma generates a durable clinical and commercial opportunity that the compressed timeline of aggressive disease cannot offer by its very nature.
The azer-cel programme spans multiple indications, and the DLBCL work remains part of it. What the current evidence shows is where the strongest data and most advanced regulatory engagement now sits. What this tells you as an investor is that the regulatory pathway most relevant to near-term programme development is the one aligned with chronic, relapsing B-cell disease.
Traditional CAR-T therapy is autologous: a patient’s own T-cells are collected through a process called leukapheresis, sent to a manufacturing facility, engineered to target cancer cells, expanded, and shipped back for infusion. That process typically takes approximately 2-4 weeks.
Azer-cel takes a different approach. It is an allogeneic CAR-T product built from healthy donor cells via the ARCUS gene-editing platform, which employs a non-integrating AAV vector to place the CD19 CAR construct directly into the TRAC locus of donor T-cells with precision. The result is an inventory-based product that can be delivered in approximately 3-5 days, according to Diamond Equity Research’s 18 June 2026 note. That figure reflects company-guided operational potential rather than a formally standardised or independently benchmarked metric.
| Feature | Azer-cel (Allogeneic) | Autologous CAR-T |
|---|---|---|
| Manufacturing Source | Healthy donor cells | Patient’s own cells |
| Gene-Editing Platform | ARCUS (non-integrating AAV vector) | Varies by product |
| Delivery Timeline | ~3-5 days (company-guided) | ~2-4 weeks |
| Patient-Specific Process | No | Yes |
The Phase 1/1b multi-centre trial (NCT03666000) is enrolling patients across a network of roughly 10 US clinical sites and 5 sites in Australia. That footprint matters for enrolment scale as the programme expands.
For investors evaluating competitive positioning, the off-the-shelf model is not a manufacturing convenience. It is a differentiation argument. In a disease where patients relapse repeatedly over years and need prompt retreatment, the logistical gap between autologous and allogeneic delivery becomes clinically meaningful. Lisocabtagene maraleucel (liso-cel) holds accelerated approval in relapsed/refractory CLL/SLL (March 2024) and relapsed/refractory FL (May 2024), establishing the competitive bar azer-cel must clear. The differentiation case rests on access speed, safety profile, and CAR-T-naive positioning in a chronic disease setting.
The efficacy data, safety profile, and regulatory signal are now established. What determines whether this Phase 1b signal translates into a genuine registrational programme comes down to three specific, trackable variables:
The thesis in mid-2026 is coherent: a 93% ORR in CAR-T-naive indolent B-cell malignancies, FDA Fast Track for CLL/SLL and MZL, an off-the-shelf allogeneic platform with a clean early safety profile, and a competitive differentiation argument grounded in delivery speed and chronic disease fit. The question the programme now needs to answer is not whether azer-cel produces responses. It is whether those responses last long enough and replicate across a larger patient population for the FDA to see a clear path to approval.
Three signals are pointing in the same direction. The 93% indolent ORR at ASCO 2026 established the efficacy case. The FDA’s Fast Track designations for CLL/SLL and MZL confirmed that the regulatory system sees alignment between azer-cel’s strongest data and an area of genuine unmet need. The off-the-shelf allogeneic platform, with zero Grade 3 or higher CRS and no GVHD to date, provides the delivery and safety characteristics that fit a chronic, relapsing patient population.
That coherence is real, and it is unusual at the Phase 1b stage. But the programme’s most consequential milestones are ahead, not behind. Durability data across indolent subtypes, expanded cohort sizes, and the design of a registration-directed study will determine whether this early signal converts into a genuine approval pathway. The data reported so far is Phase 1b with small patient numbers in some subtypes. What the evidence supports right now is a well-defined thesis with clearly trackable milestones; what it does not yet support is certainty about the outcome.
For investors wanting a structured framework for interpreting the full signal cluster, our dedicated guide to reading ASX biotech milestones examines how oral presentation selection, Fast Track designation, and Type C meeting outcomes each translate into distinct levels of regulatory confidence in a pre-revenue biotech programme.
This article is for informational purposes only and should not be considered financial advice. Investors should conduct their own research and consult with financial professionals before making investment decisions. Forward-looking statements regarding regulatory pathways, clinical outcomes, and programme milestones are subject to change based on trial results, regulatory decisions, and market developments.
Marginal zone lymphoma is a slow-growing B-cell lymphoma arising in the marginal zone of lymphoid tissue, characterised by a chronic relapsing pattern that can span years or decades rather than progressing rapidly like aggressive subtypes such as DLBCL.
Azer-cel achieved a 93% overall response rate across 14 evaluable CAR-T-naive indolent patients at the 2026 ASCO Annual Meeting, compared to a 67% ORR in DLBCL patients within the same 24-patient dataset.
Fast Track designation opens four pathways for Imugene: more frequent FDA communication, rolling submission review, and potential eligibility for Accelerated Approval and Priority Review; it does not lower the efficacy or safety bar required for eventual approval.
Unlike autologous CAR-T products, which require collecting and engineering a patient's own cells over approximately 2-4 weeks, azer-cel is built from healthy donor cells using the ARCUS gene-editing platform and can be delivered in approximately 3-5 days based on company-guided estimates.
The three most critical variables are durability of response at 6, 12, and 18-month follow-up in indolent cohorts; expansion of enrolment across MZL, CLL/SLL, FL, and WM subtypes to move beyond signal-generating data; and the design of a Phase 2/3 or Accelerated Approval study arising from Fast Track FDA interactions.




