
What Micron vs Apple Reveals About AI Spending and Returns
1 hr ago

A US$12.0 billion drug class has a known ceiling. Within the BTK inhibitor class, a portion of patients will, over time, stop responding or become unable to tolerate their therapy, and when that happens, subsequent treatment options are narrow and the situation is urgent.
BTKis are oral targeted therapies whose mechanism centres on blocking Bruton’s tyrosine kinase, a signalling protein that sits at the heart of B-cell survival. They have earned their place as a genuine clinical advance across chronic lymphocytic leukaemia/small lymphocytic lymphoma (CLL/SLL), mantle cell lymphoma (MCL), marginal zone lymphoma (MZL), and Waldenström macroglobulinemia (WM), and the revenue figures reflect that clinical value. But the gap is not a failure of the class; it is a biological inevitability. By the time patients have progressed through BTKi therapy, they carry a heavy prior treatment burden, and time matters: autologous CAR-T, the most potent available next-line tool, carries a manufacturing window of approximately 2-4 weeks during which disease continues to advance.
Here is the analytical framework for understanding why the allogeneic off-the-shelf model may be structurally better suited to this patient population, what the azer-cel Phase 1b data suggest so far, and what the opening of Cohort 3 means in practice for the BTKi-relapsed or refractory gap.
BTK inhibitors, including ibrutinib, acalabrutinib, and zanubrutinib, work by blocking Bruton’s tyrosine kinase within the B-cell receptor signalling pathway. Without BTK signalling, malignant B cells lose a survival mechanism they depend on. That mechanism is effective enough to have made BTKis the established oral standard of care across four B-cell malignancy types:
Market context: Industry estimates place the global BTKi market at approximately US$12.0 billion (2025 estimate, per Imugene ASX announcement 22 May 2026; figures vary by source). This reflects the scale of the BTKi-treated patient universe, not a commercial projection for any single therapy.
That scale tells you the population exposed to BTKi therapy is large. The resistance ceiling tells you a meaningful subset of that population will eventually need something else.
Resistance mechanisms include acquired BTK mutations and PLCγ2 mutations, as well as progressive disease on covalent BTKis. Intolerance-driven discontinuation is a separate but similarly consequential driver. Each of these pathways generates a distinct cohort of patients with relapsed or refractory B-cell malignancies who carry prior BTKi exposure and require a subsequent line of therapy, and the question is what that next line looks like.
Peer-reviewed characterisation of BTK resistance mechanisms identifies acquired BTK mutations at C481S and related sites, together with PLCγ2 mutations, as the dominant molecular drivers of treatment failure in CLL patients, a pattern that extends across the broader B-cell malignancy spectrum where BTKis are standard of care.
To understand why logistics matter clinically, walk through the autologous CAR-T manufacturing sequence step by step:
Vein-to-vein time, the elapsed period between cell collection and treatment delivery, spans approximately 2-4 weeks for autologous approaches. For a patient carrying a heavy prior treatment burden who has progressed through BTKi therapy, that window is not a scheduling inconvenience, because tumour biology does not pause for logistics, and disease progression does not wait for manufacturing to complete.
Academic analysis of autologous CAR-T manufacturing timelines confirms that vein-to-vein durations of two weeks or longer are typical under conventional production protocols, with manufacturing failure rates and disease progression during the wait period representing documented contributors to patient attrition before infusion.
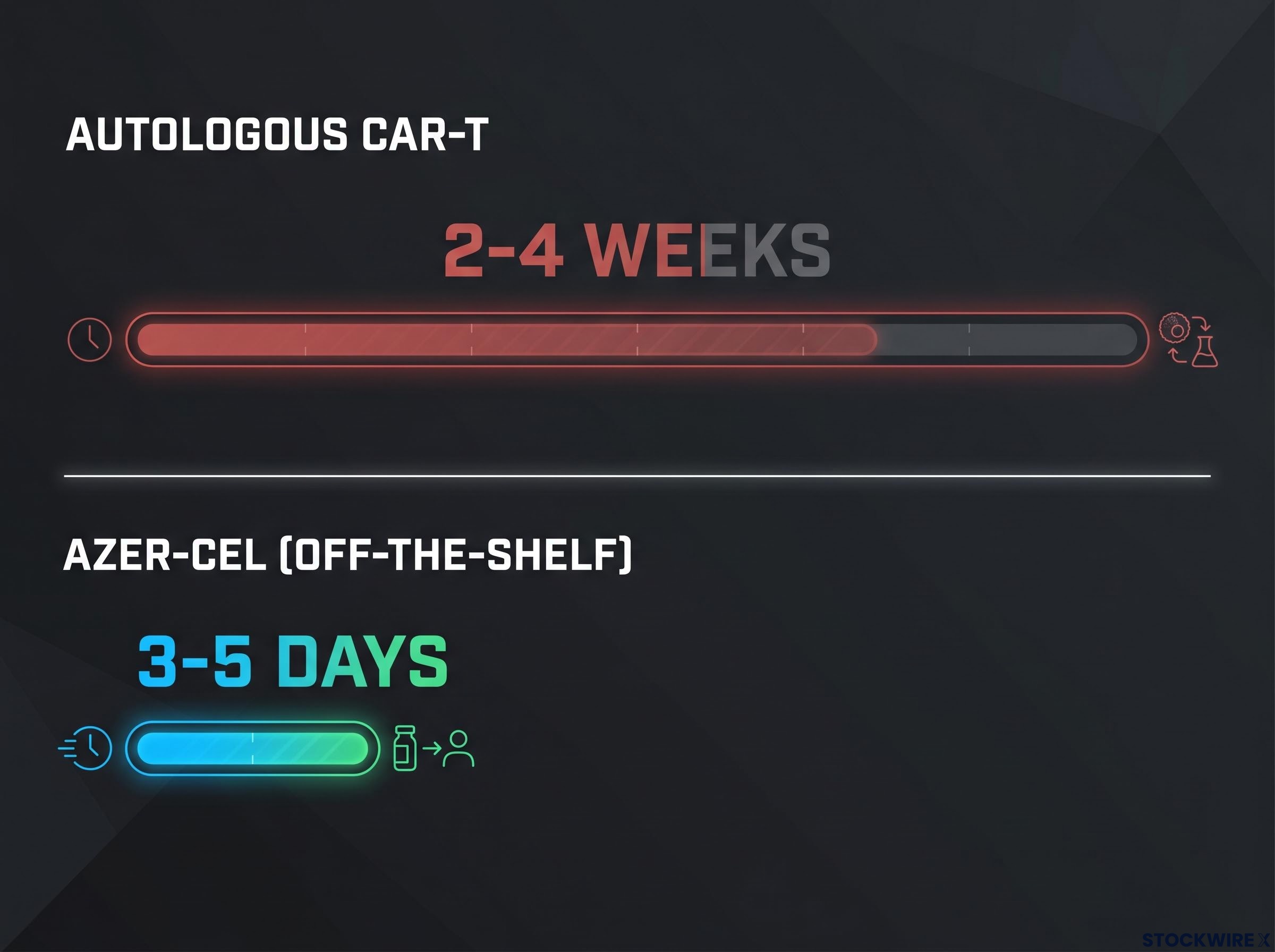
Azer-cel takes a structurally different approach. Manufactured from healthy donor T cells using the ARCUS gene-editing platform, the product is built in advance and stockpiled, removing the patient-specific manufacturing bottleneck entirely.
Working with a non-integrating adeno-associated virus (AAV) vector, the ARCUS platform places the CD19-targeting CAR construct directly into the TRAC locus of the donor T cells. This locus is deliberately selected because integration at this site disrupts and removes the donor cell’s endogenous T-cell receptor (TCR), the structure that would otherwise drive recognition of the recipient’s tissues as foreign and trigger GVHD. By knocking out the TCR at the point of CAR insertion, the platform addresses the central immunological risk of allogeneic cell therapy. As of the ASCO 2026 presentations and Imugene ASX announcements, no GVHD events have been observed anywhere in the Phase 1b programme.
Delivery window: The azer-cel programme targets an operational window of approximately 3-5 days from treatment decision to infusion (Diamond Equity Research note, 18 June 2026); real-world turnaround times may vary.
For BTKi-relapsed or refractory patients who are heavily pre-treated and running out of time, the difference between weeks and days is where the allogeneic model’s structural advantage sits.
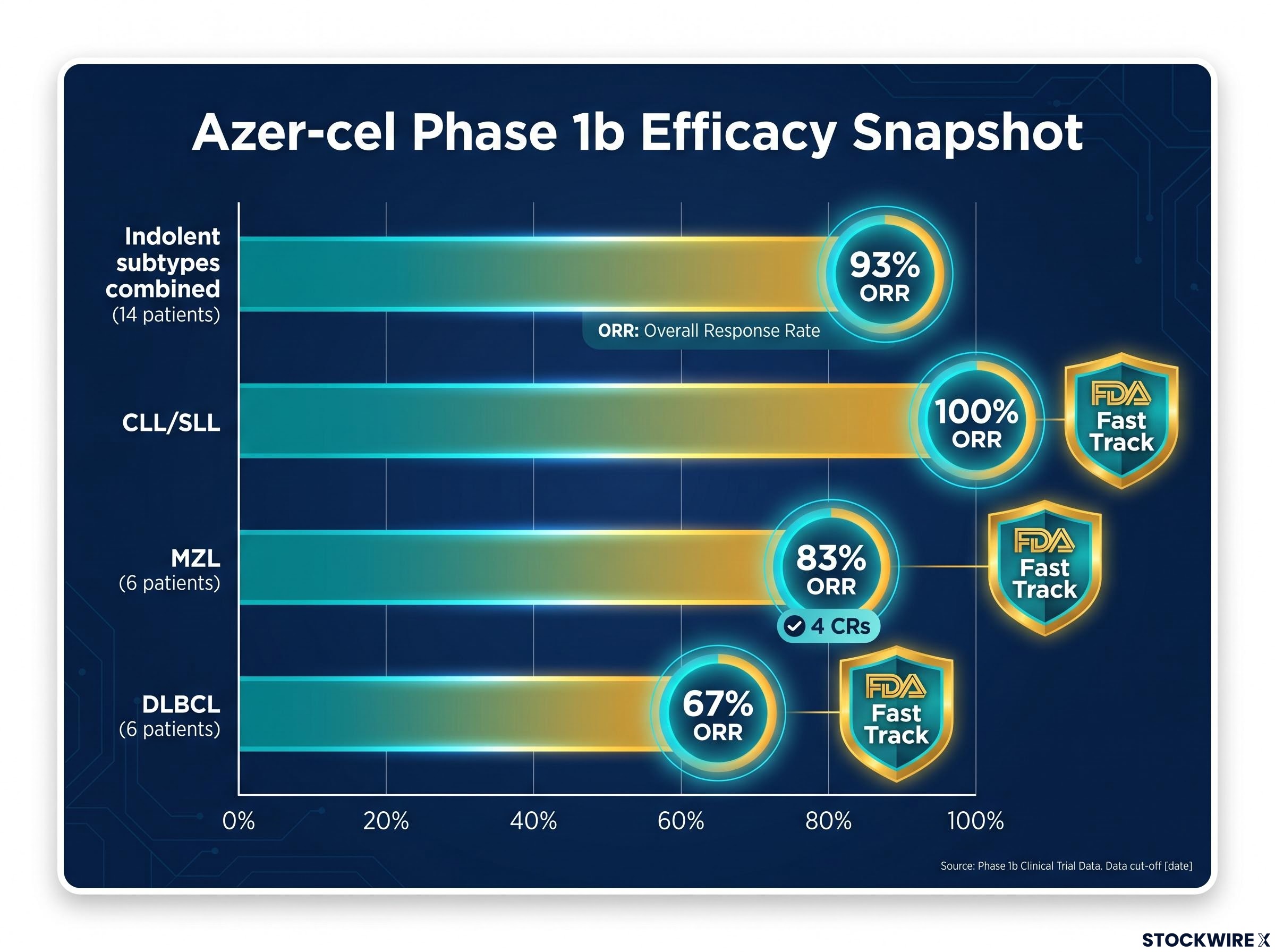
Clinical activity data for azer-cel draw on 24 efficacy-evaluable patients who were CAR-T-naïve at enrolment, spanning six B-cell malignancy subtypes, with results presented at ASCO 2026.
The standout result is the response rate across indolent subtypes: looking at those 14 evaluable patients together, the combined overall response rate (ORR), meaning the share whose disease shrank or resolved after treatment, reached 93%. The per-indication breakdown shows where that activity concentrates.
The earlier Phase 1b results from March 2026 captured the first public data cut across CAR-T-naive patients, with 100% ORR in CLL/SLL and 80% ORR in MZL, establishing the efficacy baseline that the ASCO 2026 data subsequently extended.
| Indication | Evaluable patients | ORR | FDA Fast Track |
|---|---|---|---|
| Indolent subtypes (combined) | 14 | 93% | See individual |
| CLL/SLL | Not separately specified | 100% | Yes |
| MZL | 6 | 83% (4 CRs; updated post-ASCO) | Yes |
| DLBCL (CAR-T-naïve) | 6 | 67% | Yes |
Post-ASCO, the MZL figures were revised to show an 83% ORR with 4 complete responses across 6 evaluable patients, as reported in the Diamond Equity Research note of 18 June 2026. The FDA Fast Track designations covering relapsed/refractory CLL/SLL and relapsed/refractory MZL were confirmed in Imugene‘s ASX announcement of 22 May 2026.
Safety signal: Across the complete Phase 1b programme, no patient has experienced a Grade 3 or higher cytokine release syndrome (CRS) event, a serious inflammatory reaction that can occur when large numbers of CAR-T cells activate simultaneously. This holds across all cohorts reported to date (ASCO 2026 presentation, Imugene ASX announcements, Diamond Equity Research note 18 June 2026).
What that 93% combined ORR in indolent subtypes tells you is that the platform already works across the same indications where BTKi is standard of care. The question Cohort 3 is designed to answer is whether it also works in patients who have already been through BTKi therapy.
For investors wanting the full picture on disease-specific toxicity signals, our deep-dive into azer-cel’s DLBCL safety profile covers the elevated Grade 3 or higher ICANS rate observed in DLBCL patients specifically, a signal that is distinct from the indolent subtype safety data reviewed here and that Phase 3 enrolment will need to resolve.
The combination rationale draws on accumulating preclinical and early clinical data pointing to a role for BTK inhibition that extends beyond direct tumour cytotoxicity. The emerging picture is that blocking BTK may also blunt immunosuppressive activity within the tumour microenvironment, the tissue surrounding the cancer, in ways that could support more robust CAR-T cell expansion and persistence once the engineered cells are infused.
That positions the two therapies as additive and complementary rather than competitive:
Cohort 3 enrols patients who are BTKi-relapsed or refractory, meaning their disease has already progressed on or become refractory to BTKi. The BTKi component in the combination is not being used as the primary treatment for a responding patient; it is being evaluated for its immunomodulatory role. That distinction matters.
The investor frame shifts here. This is not “azer-cel as an alternative to BTKi.” It is “azer-cel as a potential complement to BTKi in patients whose disease has moved beyond what BTKi can control alone.” That is a meaningfully different clinical and commercial position.
The combination rationale is based on emerging evidence and company communications. Cohort 3 is investigational and designed to test whether the biological hypothesis translates clinically.
Milestone: Cohort 3 has begun enrolment, with the opening patient, an individual with MCL who had previously been treated with a BTKi, receiving their infusion at Baylor University Medical Center in Texas (Diamond Equity Research note, 18 June 2026).
This is an operational milestone, not a clinical outcome. The trial is now active, not yet data-generating in a reportable sense. Specific Cohort 3 details may not yet be fully reflected in public registries such as ClinicalTrials.gov; the milestone is based on third-party analyst coverage and company communications.
The clinical trial network supporting Cohort 3 enrolment spans 15 investigational sites distributed across two countries:
For this population, azer-cel’s 3-5 day anticipated delivery window carries particular weight. Patients reaching this line of therapy carry a substantial prior treatment history, and the off-the-shelf logistics argument built earlier in this analysis applies most directly here, where treatment delay carries the greatest clinical consequence.
Investors following Imugene (ASX: IMU) need a concrete set of milestones to separate meaningful progress from noise as Cohort 3 advances. Four watchpoints carry the most weight:
The FDA Fast Track designations for relapsed/refractory CLL/SLL and MZL were secured on the back of the same Phase 1b efficacy data reviewed here, and the designation unlocks rolling review eligibility and more frequent agency engagement ahead of any registrational trial submission.
These watchpoints are forward-looking. Specific BTKi combination cohort details are not yet fully mirrored in ClinicalTrials.gov, and none of these signals represent already validated outcomes.
Azer-cel is an early-phase asset. Phase 1b data are preliminary and not sufficient to establish efficacy or safety for regulatory approval purposes. Development-stage biotech investing carries the possibility of total capital loss. This analysis does not constitute financial or investment advice. Investors should seek independent professional financial advice before making any investment decisions.
The development trajectory follows an internally coherent clinical logic:
Each programme stage was designed to build evidentiary credibility for the next. The specific question Cohort 3 answers is one the monotherapy cohorts cannot: whether azer-cel works in patients who have already exhausted the standard-of-care BTKi class. That is the harder clinical question, and it is the one the programme has earned the right to attempt based on the Phase 1b data generated to date.
The US$12.0 billion BTKi market figure gives context for the scale of the patient population under study, not a revenue forecast for azer-cel. The asset remains in early-phase development. FDA Fast Track designations for CLL/SLL and MZL provide regulatory scaffolding already in place ahead of Cohort 3 data. All forward-looking elements carry clinical and regulatory risk, and the gap between a first patient dosed and a dataset that moves a development thesis is where the real uncertainty sits.
For readers wanting to understand the evidentiary limits in more depth, our full explainer on Phase 1b data interpretation examines the specific gap between early-phase response data and the durability, comparative efficacy, and population-size evidence required for regulatory approval decisions.
This article is for informational purposes only and should not be considered financial advice. Investors should conduct their own research and consult with financial professionals before making investment decisions.
A BTK inhibitor is an oral targeted therapy that blocks Bruton's tyrosine kinase, a signalling protein essential for malignant B-cell survival. The class is the established standard of care across CLL/SLL, mantle cell lymphoma, marginal zone lymphoma, and Waldenström macroglobulinemia, generating approximately US$12.0 billion in global annual revenue.
Resistance to BTK inhibitors develops primarily through acquired mutations at the BTK C481S site and related positions, as well as PLCγ2 mutations, which allow malignant B cells to survive despite the drug. Intolerance-driven discontinuation is a separate but equally significant driver that forces patients off therapy before disease progression occurs.
Autologous CAR-T is manufactured from the patient's own T cells, requiring a vein-to-vein production window of approximately 2-4 weeks during which disease continues to advance. Off-the-shelf allogeneic CAR-T like azer-cel is manufactured from healthy donor cells in advance and stockpiled, targeting a delivery window of approximately 3-5 days from treatment decision to infusion.
Across 14 efficacy-evaluable CAR-T-naive patients with indolent B-cell malignancy subtypes, azer-cel produced a combined overall response rate of 93%, including 100% ORR in CLL/SLL and 83% ORR in MZL with 4 complete responses across 6 evaluable patients. No patient in the full programme experienced a Grade 3 or higher cytokine release syndrome event, and no GVHD events were observed.
Cohort 3 tests azer-cel in combination with a standard-of-care BTK inhibitor in patients whose disease has already progressed on or become refractory to BTKi therapy, evaluating whether the BTKi component plays an immunomodulatory role that supports CAR-T cell activity. The cohort is enrolling across 15 investigational sites, 10 in the United States and 5 in Australia, with the first patient dosed at Baylor University Medical Center in Texas.




