Why Neither Property nor ETFs Always Wins Against Inflation
11 hrs ago

A therapy that produces a response is not the same as a therapy that sustains one. That distinction sounds academic until you watch a patient’s remission unravel three months after an initially promising CAR-T infusion. It is now the single most important design question shaping how the next generation of cell therapies are being built.
Imugene Limited crystallised that question with a concrete clinical step this year: a patient with mantle cell lymphoma at Baylor University in Texas, who had previously exhausted BTK inhibitor (BTKi) options, became the first to be dosed in a new BTKi combination cohort within the azer-cel programme. This is not a routine trial amendment. It is a deliberate test of whether a well-validated drug class can solve the durability problem that has constrained CAR-T outcomes across the field.
Here is what you need to understand: why combination therapy has moved from optional add-on to central design priority in CAR-T development, what the science behind this specific combination actually involves, and what that framework means when you are evaluating clinical-stage ASX biotech stocks with cell therapy exposure.
Before you can assess the BTKi combination cohort, you need a clear picture of the asset it is built on. Azer-cel is an allogeneic (off-the-shelf) anti-CD19 CAR-T cell therapy, meaning it is manufactured from donor cells rather than individually from each patient’s own cells. It was originally developed by Precision BioSciences and is now being advanced by Imugene in a Phase 1/1b programme targeting relapsed and refractory B-cell malignancies, cancers of the white blood cells that have come back or stopped responding to prior treatment.
Key programme facts for orientation:
The Phase 1b basket study results reported in March 2026 provided the monotherapy foundation the combination cohort is now built on, with 100% overall response rates in CLL/SLL patients and 80% in marginal zone lymphoma across a heavily pre-treated population enrolled at 15 sites across the US and Australia.
The FDA Fast Track designation criteria require that a therapy address a serious condition and demonstrate potential to fill an unmet medical need, with qualifying programmes receiving more frequent agency meetings, rolling review eligibility, and an expedited path toward priority review consideration.
The monotherapy signal is what makes the combination cohort credible rather than speculative:
For investors wanting the original news context around this clinical milestone, our dedicated guide to the azer-cel BTKi combination cohort covers the trial design, the addressable patient population across mantle cell lymphoma, follicular lymphoma, and CLL, and the commercial framing around the BTKi-relapsed market that Imugene has cited.
The most recent data cut, reported ahead of the ASCO 2026 oral presentation in May, showed an 81% overall response rate across six subtypes in CAR T-naive patients, with four indications including MZL, CLL, follicular lymphoma, and Waldenstrom macroglobulinemia each reaching 100% response rates in evaluable patients.
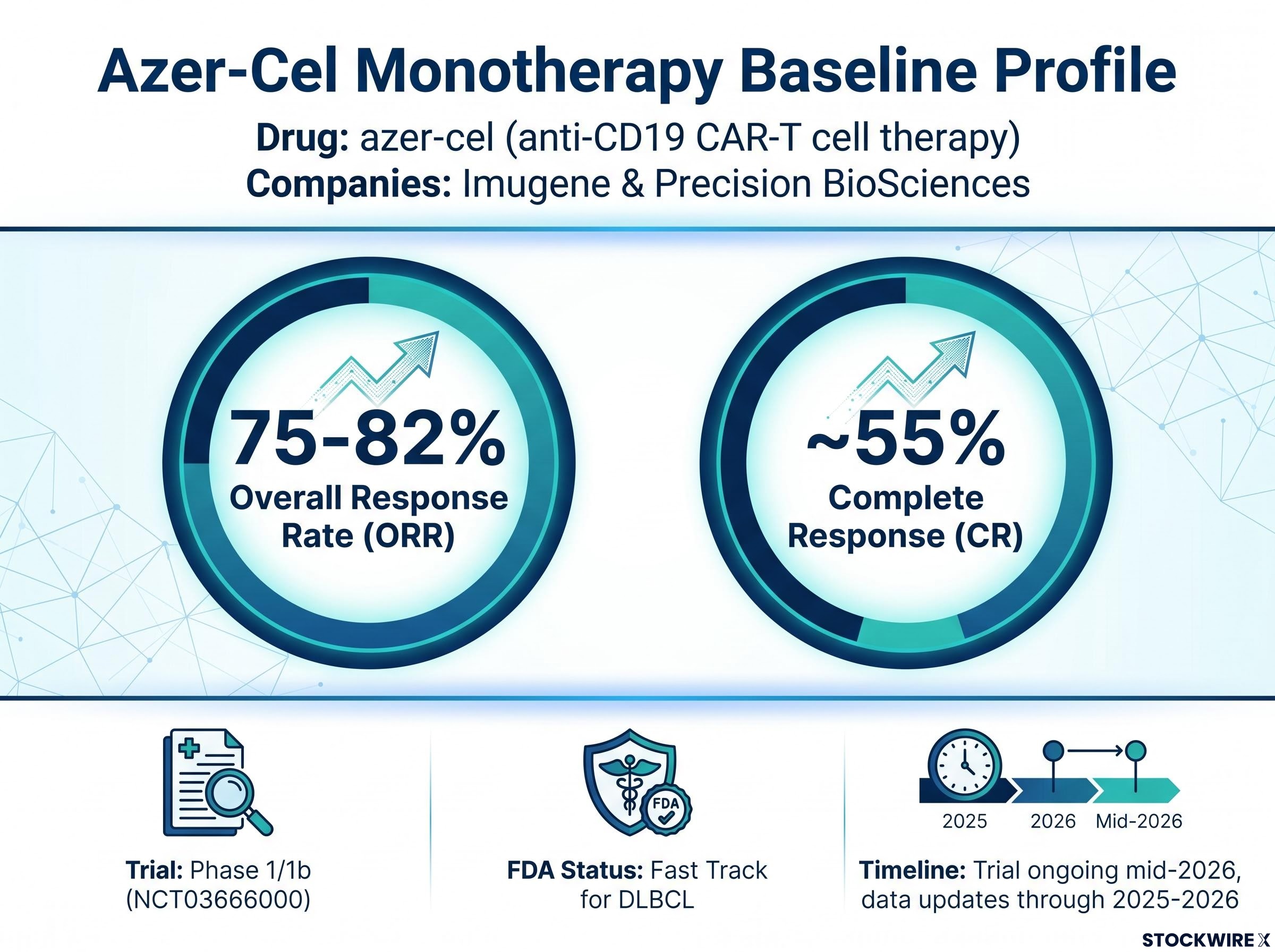
That baseline matters. A combination arm built on a weak single-agent signal would be a red flag for you as an investor. One built on 75-82% ORR in refractory patients is a materially different proposition; it tells you the BTKi addition is being tested to enhance an already functioning therapy, not to rescue a struggling one.
The pattern has repeated across the cell therapy field for years. A CAR-T programme reports impressive early response rates. Patients who had run out of options are achieving complete remissions. The data look strong.
Then the follow-up data arrive, and a meaningful proportion of those remissions have not held. The therapy engaged the target. It produced a response. But it did not maintain it.
The explanation, in most cases, is T-cell exhaustion: the progressive loss of functional potency in engineered CAR-T cells over time. Your infused cells gradually lose their ability to find, attack, and destroy cancer cells. The therapy that worked in month one may be functionally spent by month six.
The field’s defining challenge is no longer whether CAR-T can produce a response. It is whether CAR-T can be engineered to sustain one.
What researchers have identified is that the type of T cell matters as much as the T cell’s initial activity. CAR-T cells that maintain a stem-like or memory phenotype (a more youthful, self-renewing state) tend to persist longer and maintain function. Exhausted effector cells (cells that have been heavily activated and are burning out) lose potency relatively quickly.
For you, this reframes how to read interim clinical data. A high ORR at an early data cut is encouraging, but it is a partial answer. The question that determines long-term commercial value is whether those responses hold, and T-cell exhaustion is the primary reason many do not.
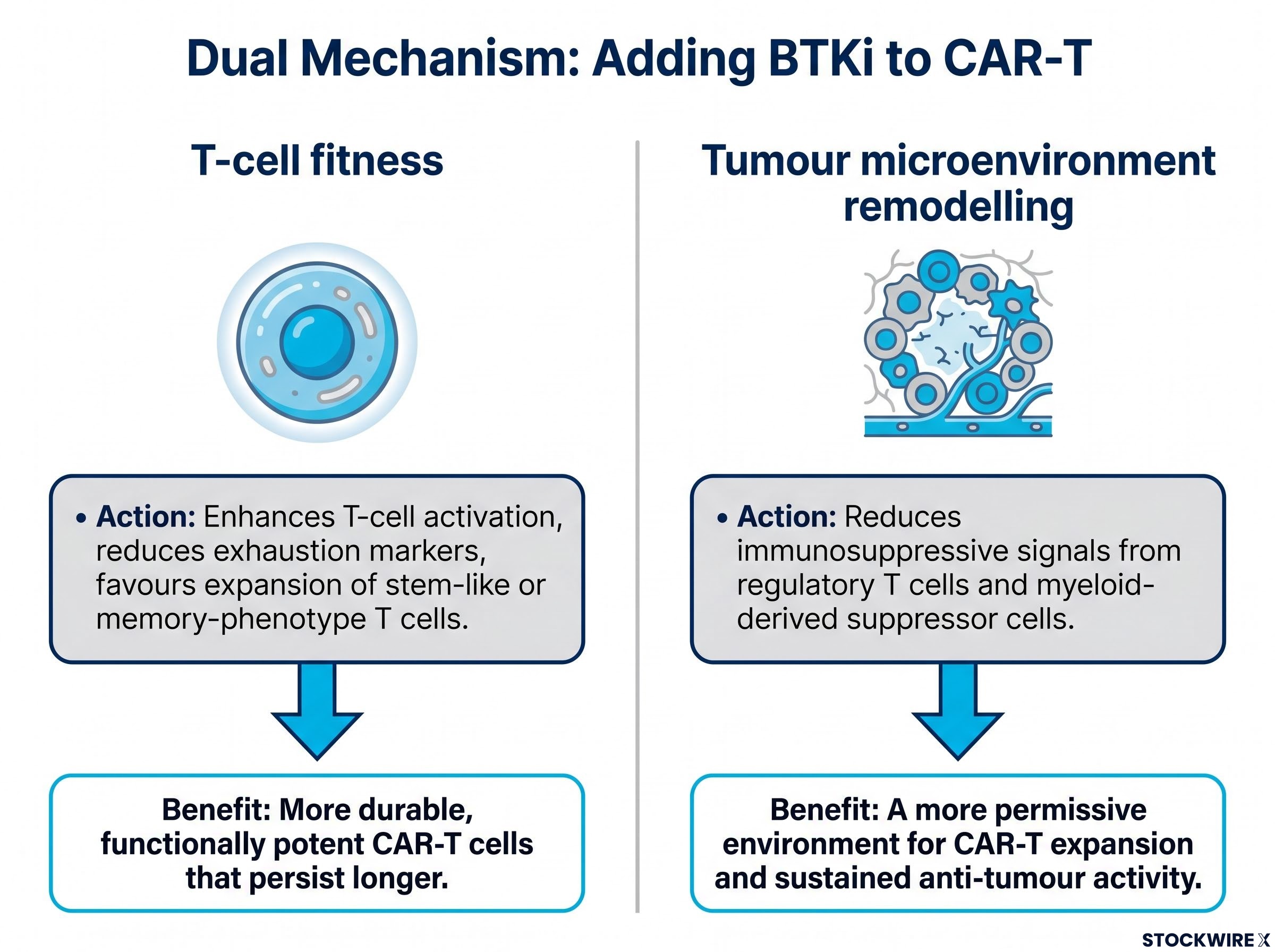
The scientific rationale for adding a BTK inhibitor to azer-cel rests on two overlapping mechanisms. Understanding both gives you the framework to assess whether this combination is grounded in real biology or is simply a trial design aimed at generating attention.
BTK inhibitors, a class of drugs including ibrutinib, acalabrutinib, and zanubrutinib, are best known for blocking a signalling pathway (Bruton’s tyrosine kinase) that malignant B cells rely on to survive. But their effects extend beyond the tumour itself.
| Mechanism | What BTKi does | Expected CAR-T benefit |
|---|---|---|
| T-cell fitness | Enhances T-cell activation, reduces exhaustion markers, favours expansion of stem-like or memory-phenotype T cells | More durable, functionally potent CAR-T cells that persist longer in the body |
| Tumour microenvironment remodelling | Reduces immunosuppressive signals from regulatory T cells and myeloid-derived suppressor cells | A more permissive environment for CAR-T expansion and sustained anti-tumour activity |
The two mechanisms work simultaneously. The BTKi is not just improving the CAR-T cells themselves; it is also improving the biological environment those cells operate in. The combined effect is therefore expected to produce responses that are both deeper and more sustained, going beyond what a straightforward additive interaction would predict.
Field-level evidence supports the rationale, even though azer-cel-specific combination data has not yet been reported:
These are field-level findings, not azer-cel results. But they are what make the combination hypothesis scientifically credible rather than speculative, and that distinction matters when you are assessing whether a clinical programme’s design is grounded in evidence or reaching for headlines.
Here is the detail that might seem counterintuitive at first. The first patient in the combination cohort is someone whose cancer already failed to respond to BTK inhibitor therapy. Why would you add a drug that already did not work?
The answer is that the cohort is not testing whether the BTKi can kill the tumour. It is testing something more specific and more valuable.
BTKi resistance, driven primarily by BTK C481S mutations or alternative pathway activation, is a growing clinical problem. Patients with CLL, mantle cell lymphoma, and related diseases who progress through sequential BTKi lines face poor outcomes and limited treatment alternatives.
The logical sequence makes the design choice clear:
For you as an investor, this patient selection is a signal of scientific rigour, not commercial conservatism. It sets up the most interpretable possible dataset. Clean tests produce the data that regulators, potential partners, and the broader field can act on with confidence.
It also opens two addressable populations rather than one. If the combination works in patients who have already failed BTKi, the logical next step is testing it in earlier treatment lines where BTKi is standard of care and patient volumes are substantially higher.
The commercial context for this combination is not hypothetical. BTK inhibitors already occupy entrenched standard-of-care positions across multiple blood cancer indications:
The global BTKi market is estimated at approximately US$11.6 billion in 2026, though this figure should be treated as an industry estimate rather than a confirmed valuation.
That market figure matters less as a revenue projection and more as a signal of where patient flows already exist. A CAR-T that can be safely combined with BTKi, or used effectively after BTKi failure, plugs into existing treatment pathways and clinical infrastructure. It does not need to create a new market from scratch.
For ASX investors evaluating clinical-stage biotech exposure, that distinction is a material risk factor. The difference between a therapy building toward an established commercial channel and one requiring de novo market creation shapes your timeline, your downside, and the probability of partnership interest. Imugene’s approach, establishing monotherapy safety and activity before adding a carefully chosen combination arm alongside one of oncology’s most commercially active drug classes, keeps the regulatory pathway clean and positions the asset within a large, well-defined addressable market.
The ASX CAR-T development landscape extends beyond B-cell malignancies: AdAlta’s BZDS1901 programme reported a 50% overall response rate in advanced mesothelioma at its highest doses in March 2026, with a manufacturing process under two days and no viral vectors required, illustrating how different design priorities are shaping distinct niches within the same asset class.
No safety or efficacy data from the BTKi combination cohort has been reported yet. This cohort is at an early, exploratory stage, and describing it in stronger terms would go beyond what the current evidence supports. Characterising the programme this way is not a limitation; it reflects the kind of honest scientific communication that builds credibility with investors who can distinguish genuine rigour from promotional framing. The programme is structured to yield data that can bear scrutiny, rather than to generate headline claims ahead of the evidence.
When the first combination readouts arrive, here are the three variables that will tell you the most:
The risk structure here is asymmetric, and that matters for how you position your expectations. If the combination cohort shows limited benefit, the monotherapy data remain intact. Azer-cel’s path in salvage large B-cell lymphoma and related indications does not depend on the combination hypothesis proving out. The monotherapy programme continues regardless.
The absence of combination data right now is not a gap you need to fill with speculation. It is an opportunity to build your understanding of the programme’s architecture, so that when the next readout arrives, you know exactly what questions it is answering.
This article is for informational purposes only and should not be considered financial advice. Investors should conduct their own research and consult with financial professionals before making investment decisions. These statements regarding future clinical outcomes are speculative and subject to change based on trial results and company performance.
T-cell exhaustion is the progressive loss of functional potency in engineered CAR-T cells over time, causing initially effective therapies to lose their ability to destroy cancer cells within months of infusion. It is the primary reason many early CAR-T responses do not hold at follow-up, making it the central design challenge for next-generation cell therapies.
Azer-cel is an allogeneic (off-the-shelf) anti-CD19 CAR-T cell therapy developed by Precision BioSciences and now advanced by Imugene in a Phase 1/1b programme for relapsed and refractory B-cell malignancies. Its most recent data cut, reported ahead of ASCO 2026, showed an 81% overall response rate across six subtypes in CAR T-naive patients, with four indications each reaching 100% response rates in evaluable patients.
Enrolling BTKi-resistant patients removes the drug's direct anti-tumour effect from the equation, meaning any clinical benefit observed must come from the BTKi's immunological effects on the CAR-T cells and the tumour microenvironment. This makes the trial's scientific test clean and unambiguous, producing data that regulators and potential partners can act on with confidence.
BTK inhibitors work on two overlapping mechanisms: they enhance T-cell activation, reduce exhaustion markers, and favour stem-like or memory-phenotype T cells, while simultaneously reducing immunosuppressive signals in the tumour microenvironment. The combined effect is expected to produce CAR-T responses that are both deeper and more sustained than monotherapy alone.
The three key variables are response depth in BTKi-resistant patients, the tolerability profile of the combination relative to the monotherapy arm, and whether early signals show CAR-T cells persisting longer or maintaining function more effectively than in monotherapy historical data. Crucially, if the combination cohort shows limited benefit, the monotherapy programme continues independently and azer-cel's path in salvage large B-cell lymphoma remains intact.