
Brent Falls 3.3% as Trump Signals Imminent Iran Peace Deal
13 hrs ago

An 81% overall response rate across six cancer subtypes in heavily pre-treated patients is the kind of headline number that moves biotech stocks. Whether it should is a more complicated question.
Imugene presented Phase 1b expansion cohort data for its allogeneic CAR-T candidate azer-cel (azercabtagene zapreleucel) at ASCO 2026 on 9 June 2026, the same day the company announced two new FDA Fast Track Designations for relapsed/refractory chronic lymphocytic leukaemia (CLL) and marginal zone lymphoma (MZL). For Australian investors tracking the ASX-listed company, the confluence of a major oncology conference readout and fresh regulatory designations in a single news cycle warrants careful unpacking.
This article breaks down the ASCO data, explains what the FDA designations actually confer, and maps out the clinical and commercial questions that will determine whether yesterday’s milestones translate into long-term value.
The headline figure is genuinely striking. Across 19 evaluable patients in the ASCO 2026 Abstract 7012 dataset, azer-cel delivered an overall response rate (ORR) of 81%, with a complete response (CR) rate of 31%.
81% overall response rate at Day 28 across six relapsed/refractory B-cell malignancy subtypes in heavily pre-treated, CAR-T-naïve patients (ASCO 2026 Abstract 7012, 19 evaluable patients).
The responses spanned all six B-cell malignancy subtypes enrolled: diffuse large B-cell lymphoma (DLBCL), MZL, CLL, primary central nervous system lymphoma (PCNSL), follicular lymphoma (FL), and Waldenström’s macroglobulinaemia (WM). Some 21% of enrolled patients had received more than four prior lines of therapy before entering the study.
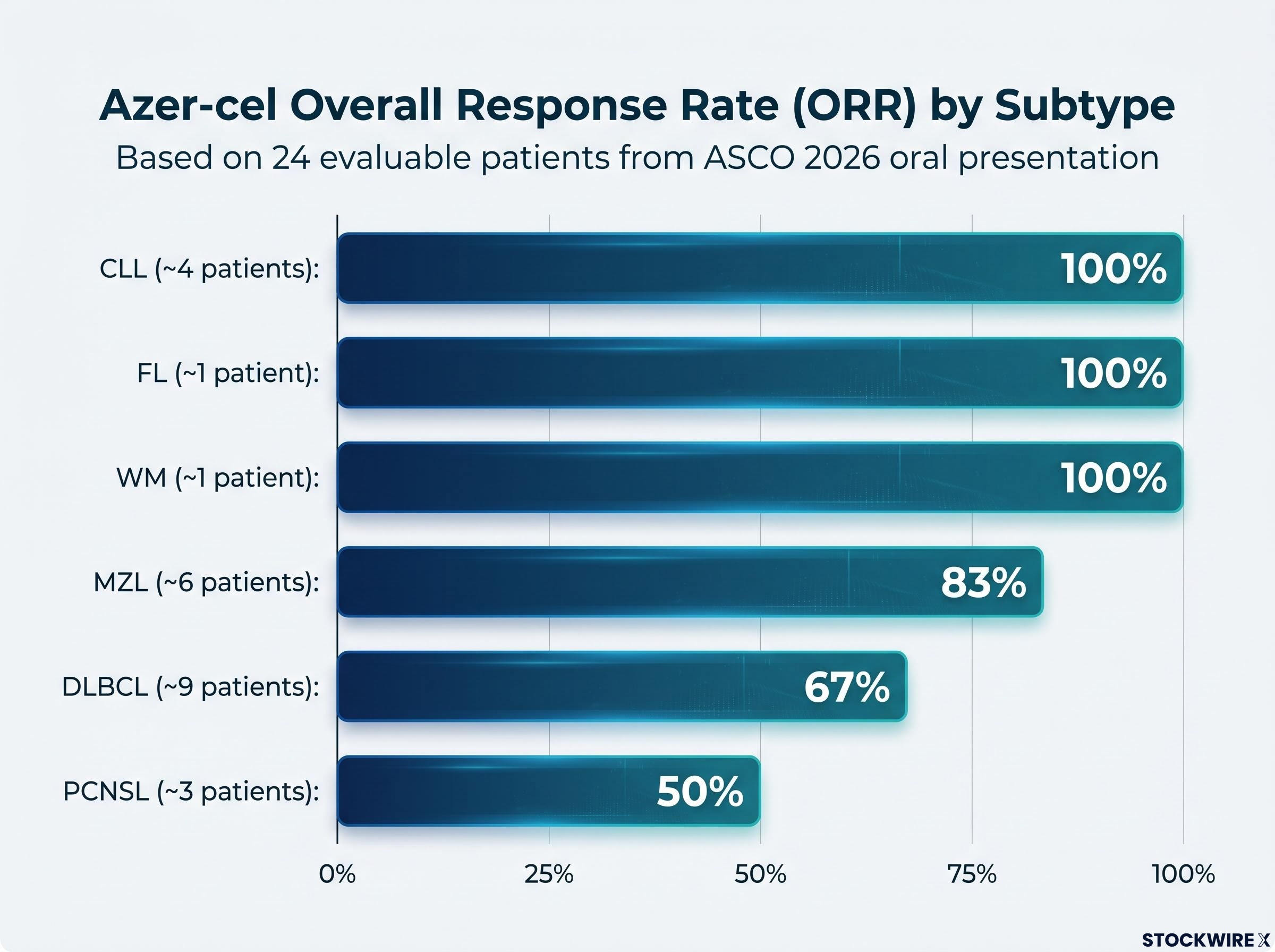
An updated oral presentation dataset, reflecting 24 evaluable patients out of 25 treated, provided the following subtype-level response rates:
| Cancer Subtype | Approximate Patient Count | ORR |
|---|---|---|
| DLBCL | ~9 | 67% |
| MZL | ~6 | 83% |
| CLL | ~4 | 100% |
| PCNSL | ~3 | 50% |
| FL | ~1 | 100% |
| WM | ~1 | 100% |
The difference between the 19-patient abstract and the 24-patient oral presentation reflects more recent enrolment data captured after the abstract submission deadline. The primary disease assessment was conducted at Day 28 post-infusion, meaning durability data is still maturing. With subgroup sizes in the single digits for several subtypes, a handful of additional patients could shift these figures substantially. The signal is encouraging; the sample size demands caution.
A pre-ASCO interim readout published in late May 2026 captured the 16-patient dataset that preceded both the abstract and oral presentation figures, providing a third data snapshot that illustrates how quickly the trial has been enrolling across its six B-cell malignancy subtypes.
CAR-T therapy works by engineering immune cells to recognise and attack cancer. The distinction that matters for azer-cel is how those cells are sourced.
Azer-cel is an allogeneic, off-the-shelf therapy targeting CD19-positive B-cell malignancies, administered in combination with low-dose IL-2. The trial includes both CAR-T-naïve patients and those who had relapsed after prior autologous CAR-T therapy, a population with very limited treatment options.
The format carries potential advantages in manufacturing speed, access, and cost if the clinical profile holds at scale. It also enters a space where approved autologous CD19 CAR-T products already exist in DLBCL, alongside emerging allogeneic competitors. Whether azer-cel is solving a genuine access problem or offering incremental differentiation in a crowded field is not yet clear, but it is the right question for investors to track.
The competitive landscape for allogeneic CAR-T development was on display at ASCO 2026 more broadly, with Chimeric Therapeutics reporting an 82% disease control rate for its CDH17 CAR-T programme across 11 evaluable patients, a result that highlights both the sector’s collective momentum and the difficulty of drawing direct efficacy comparisons across trials with different target antigens, patient populations, and disease contexts.
Efficacy numbers attract attention. Safety data determines whether a therapy survives the transition from a small trial to a registrational programme.
The key safety metrics from the Phase 1b dataset:
The ASTCT consensus grading for CRS and ICANS establishes the uniform criteria by which grades 1-2 CRS is classified as manageable and grade 3-4 events are flagged as requiring escalated intervention, the same framework regulators apply when evaluating whether a CAR-T programme’s toxicity profile is acceptable for advancement to a larger pivotal population.
One Grade 4 ICANS event has been observed across approximately 25 treated patients, the sole high-grade safety signal in the current dataset.
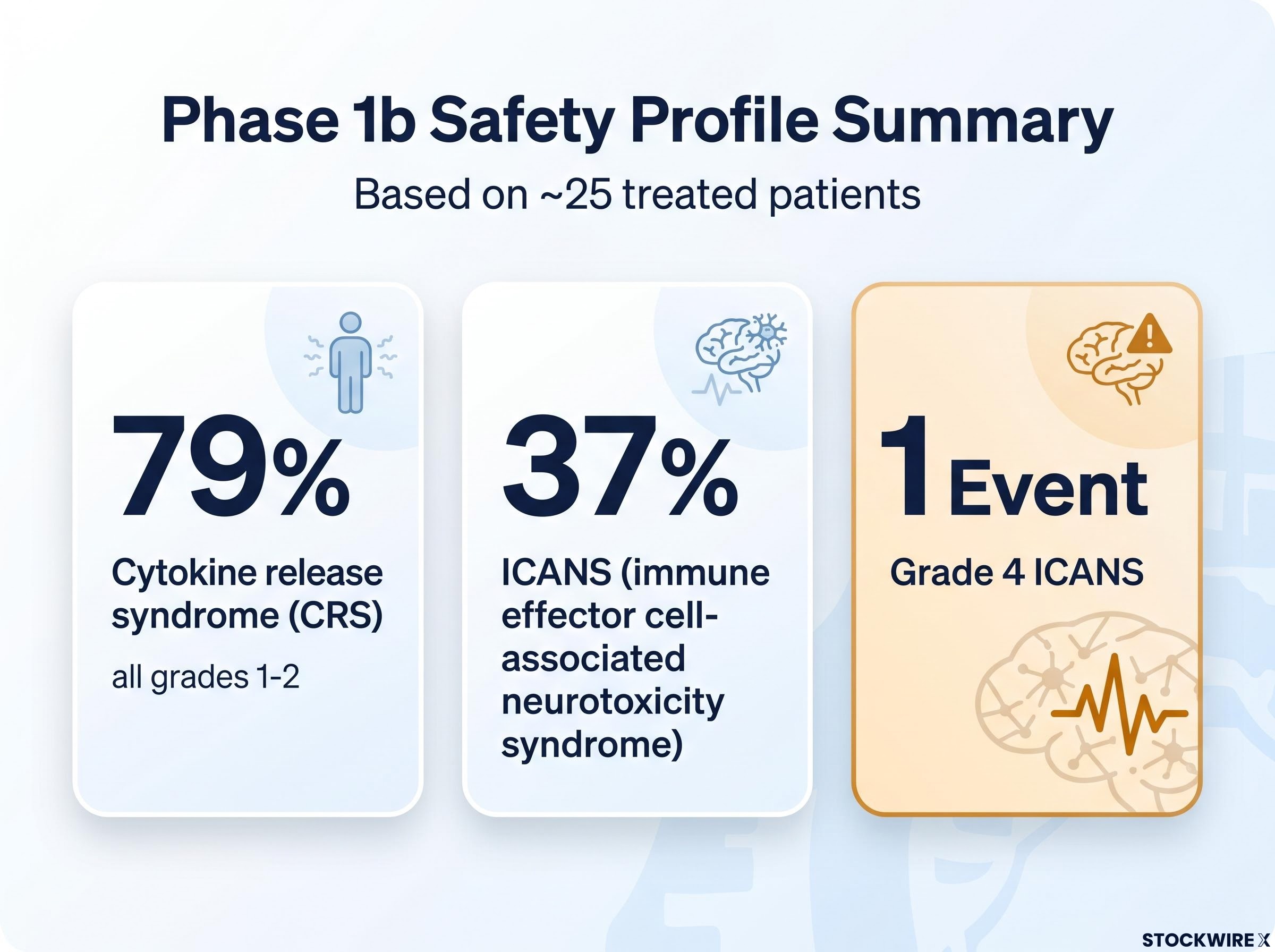
A single high-grade neurotoxicity event in roughly 25 patients is not alarming in isolation. The company has described the overall safety profile as consistent with the broader CAR-T class. The question is whether ICANS frequency and severity remain stable as patient numbers increase. Phase 1b-to-pivotal transition risk concentrates here: what appears manageable in 25 patients may look different in 250.
Imugene now holds three FDA Fast Track Designations for azer-cel. The DLBCL designation was granted in March 2025. Two additional designations, for CLL and MZL, were reported by Imugene in an ASX announcement on 9 June 2026, though these have not been independently verified in publicly indexed sources at the time of writing.
Rolling review eligibility is among the more commercially significant benefits, allowing Imugene to submit completed sections of a future Biologics License Application as clinical data packages are finalised rather than waiting until the full programme is complete, a mechanism that can compress the pre-approval timeline by several months.
For an ASX-listed biotech targeting a pivotal trial, Fast Track carries real operational value. It is not, however, a commercial outcome.
The forward-looking catalyst sequence for Imugene centres on three threads, each at a different stage of maturity.
Scientific rationale: Pre-clinical and translational data, attributed to Dr. Blunt at ASCO 2026, suggest that prior BTK inhibitor exposure may shift T-cell phenotype toward a central memory profile, which could enhance CAR-T cell persistence. This hypothesis has not yet been confirmed in clinical data.
The BTKi cohort represents a medium- to longer-term optionality thread. Its relevance is contingent on the monotherapy data first demonstrating durable efficacy and acceptable safety at larger scale.
The ASCO 2026 presentation and the concurrent FDA designations advance the azer-cel programme meaningfully. They do not, on their own, resolve the questions that sit between a Phase 1b signal and a regulatory approval.
The outstanding variables investors should monitor:
The step-change from approximately 25 Phase 1b patients to a pivotal trial population in the hundreds represents a substantial increase in cost, complexity, and execution risk. Investors who understand which metrics to track are better positioned than those reacting to any single data point. The session at ASCO 2026 gives them a clearer map; the destination remains years away.
Binary catalyst risk of this kind, where a single trial outcome can either validate years of development spending or eliminate most of the stock’s value, is a category of investment risk that demands pre-defined position sizing and exit conditions rather than reactive decision-making at the moment of readout.
This article is for informational purposes only and should not be considered financial advice. Investors should conduct their own research and consult with financial professionals before making investment decisions. Forward-looking statements regarding clinical trial outcomes, regulatory timelines, and commercial prospects are speculative and subject to change based on market developments and company performance.
An FDA Fast Track Designation allows more frequent communication with the FDA during development and enables rolling review of a future marketing application, but it does not lower the evidentiary bar for approval or confirm a product's safety or efficacy. Imugene now holds three such designations for azer-cel, covering DLBCL, CLL, and MZL.
Azer-cel achieved an 81% overall response rate at Day 28 across 19 evaluable patients in six relapsed/refractory B-cell malignancy subtypes, with a complete response rate of 31%, based on ASCO 2026 Abstract 7012.
Allogeneic CAR-T therapy uses donor-derived cells manufactured at scale, allowing immediate availability for multiple patients from a single production batch, whereas autologous CAR-T uses each patient's own cells and requires individualised manufacturing that can take several weeks.
Cytokine release syndrome was observed in 79% of patients, all at grades 1-2, while ICANS was reported in 37% of patients overall, with one Grade 4 ICANS event recorded across approximately 25 treated patients, the only high-grade adverse event in the current dataset.
Investors should monitor 6-12 month durability data for the CAR-T-naive cohort, pivotal trial initiation targeted for 2026, early safety and efficacy readouts from the BTKi combination cohort dosed at Baylor University in May 2026, and any further capital raises beyond the existing $22.5 million placement.



